This is a post in the Politics of Care Forum. It lies in the sequence of posts about What You Can Do to Save the World, and What Doctors can Do to Save the World. It will be followed by Can Politicians Save the World – it turned out there were just too many things to draw to politicians’ attention for one post.
One
We need to reign in Technique. That means voting for politicians who understand why.
Technologies and techniques have brought us extraordinary benefits in health and wealth domains, but they are now also driving dangerous changes in the healthcare and global climates.
The dangers techniques pose cut across traditional divides between parties of the Left and Right. See The Deep NeoLiberal State. Our problems are not now with capitalism or socialism but with techniques.
We cannot Care for Health or the Environment, unless We the People regain control of our technologies and techniques.
This is not impossible. Greta Thunberg has helped mobilize a generation to tackle climate change.
![]()
In the 1970s and 1980s, Germans forced a pause in the development of nuclear energy.
There is now a growing awareness of Surveillance Capitalism and talk about the need to tackle the Internet Giants – see Why Silicon Valley can’t fix Itself.

The talk is mostly about the profits they make. It shouldn’t be. It should be more about the techniques they use and whether these – like SSRI antidepressants – have the potential to cause more harm than good.
As An Ugly Truth, a recent book on Facebook quotes:
So we connect more people. That can be bad if they make it negative. Maybe it costs someone a life by exposing someone to bullies. Maybe someone dies in a terrorist attack coordinated on our tools. And still we connect people. The ugly truth is that we believe in connecting people so deeply that anything that allows us to connect more people more often is de facto good.
This skips the money made out of connecting people. But even more important is that behind Facebook and related companies are a set of operant techniques that have the power to control vast swathes of our behaviour to a greater extent than anyone has ever been able to achieve before. Even if those who increasingly control us are doing so for benign or even purposes they view as neutral, there is a problem here.
We have of course had Edward Snowden for some years and now we have Pegasus.
In all these areas we have made progress in grappling with the dangers of techniques but not in Health. The Guardian and New York Times for instance who have helped break many of these stories have a blind spot when it comes to health – they are pro technique and technology. There is no questioning of Progressive Health care policies, no feel for our collective Health blind spot. Life expectancy was falling before Covid, and is falling even more so now. Population Replacement Rates are also falling. No-one is asking why.
If we have fewer people isn’t that good for the environment?
If video consults reduce petrol consumption isn’t that a good thing?
Two
A Physical Environment policy platform that does not recognize the parallel degradation within the Health Environment cannot succeed. There are many ways in which properly recognising what is going wrong in Health will add teeth to Environmental policies. Its time for Politicians concerned about Sustainability, concerned about our Future, to discover this.
There is a chance to create a message of hope and value rather than be painted as Luddite, Rationing or Anti-Progress but it needs an understanding of Health that few people – either those who complain about NeoLiberalism or those worried about Deep States – have. See the Deep NeoLiberal State.
At present Green or Sustainable HealthCare policies are aggravating the problems we have in Health. Green politicians appear to think the primary contribution they can make to Health is to clean up the environment and after that encourage innovative and evidence-based Health policies. Innovation and Evidence Based are hazard markers – See The Controlled Healthcare Opposition and The MedicoChemical and PetroChemical Twins.

Three
Ulrich Bech’s book Risk Society helped create the modern environmental movement and cement in people’s minds the hazards of the modern world.
Neither science, nor the politics in power, nor the mass media, nor business, nor the law, nor even the military are in a position to define or control risks rationally…. We are living in a world that is beyond controllability.

Shortly before Beck appeared on the scene though, the pharmaceutical industry had discovered our risky world and the marketing of risk has enabled them to increase the amount of drugs we take by over 2000 per cent and grow from a $20 billion industry to over $1.2 trillion and rising fast.

In 1980 few of us were on 1 drug per say. Now over 40% of over 45s are on 3 drugs every day of the year and over 40% of over 65s are on 5 or more drugs every day of the year.
Within healthcare – poisons (medicines) are seen as the way to manage risks. This is sold to politicians as preventive medicine.
The Zeitgeist, or something, has helped turn what were viewed as poisons into sacraments (something that can only benefit) and an increasing number of us figure we need to take Daily Meds to handle Risks in the way we once sought out Daily Communion (Eucharist), or said prayers to Mecca.
Pharmaceuticalization and financialization are now the way we manage risks – and at the moment progressive and sustainable health policies are digging this hole deeper.
Four
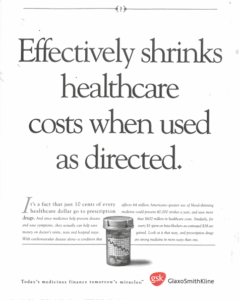
Adverts like this are directed to politicians and managers. The message – medicines like anti-hypertensives, bone thickening drugs, blood sugar reducing drugs, airway opening drugs, and drugs to reduce risky behaviours will reduce hospital admissions, making for lower costs, while at the same time being better for patients.
We now have more hospital admissions and disability caused by these drugs than we have from leaving untreated the notional risks they claim to manage.
The line in the advert here about drug prices only being 10 per cent of healthcare budgets fools policy-makers, insurers, the public and their politicians. Ten per cent of a $4 trillion budget in the United States is $400 billion. If these drugs worked, their cost would be a greater percentage of a falling budget.
We are now paying not just for the drugs, but also for the screeners whose job it is to detect risk, and the auditors and managers you need to put in place because something is going wrong with hospital admissions and escalating costs and you don’t know what. Governments and insurance premiums are paying for the salesforce for the drug – pharma don’t need to send drug reps around any more. Or even take docs out for meals.
An increasing chunk of the $3.6 trillion in the US is going on healthcare staff who are selling the drugs.
Another chunk goes on the increased admissions the drugs that are supposed to be reducing costs cause and the difficulties in effectively remedying spiral fractures of the femur caused by bone-thickcning drugs, dementia caused by hypoglycemics, rhabdomylosis caused by statins, or the mental instabilities caused by psychotropics.
Five
The amount of medicines in us is rising faster than CO2 levels are rising in the atmosphere or the amount of guns circulating in the United States.
Doctors are dishing these risk management meds out with a liberality the National Rifles Association can only envy – and they are causing more death and disability than guns are. Doctors are following a line from Donald Trump – the answer to risks is to have a good guy with a gun outside every school. They go one step further and are arming every school-child with a set of drugs.
Ask any doctor you know and medical authorities why there are no Guidelines for People, the first element of which would be a recognition that medication burdens should be contained? See What Doctors Can Do To Save the World.
If they agree Guidelines for People should take precedence over Guidelines for Diseases, which push doctors to prescribe more drugs, ask what plans there are to make this happen – or is it a matter of keeping the beaches open for the tourist season?
Six
A little over a decade ago, Deprescribing came on the radar. A paper by Garfinkel and Mangin indicated that reducing medication burden from 10 or more drugs especially in older patients to 5 or less can reduce hospitalizations, improve quality of life, and extend life expectancy.
More important than saving money and helping people feel better, Deprescribing has the potential to bring home the role of technique.
Deprescribing exposes the Nuclear Bomb problem at the heart of all techniques.
As with armaments, drugs produce an arms race. The side with the most effective weapons wins so there is no option but to compete. And weapons get more and more effective until we get to the Nuclear Bomb which is too effective to use.
Efficacy has its limits. And just as we can have bombs too effective to use, so we cannot now use all our drugs. Effectiveness starts falling off once we go above 3 drugs per day.
Getting the maximum bang for our buck means deprescribing. This is not a matter of rationing, its a matter of sustainability. And there is no place for an algorithm in sustaining what each of us might want sustaining.
This is not just a matter of overall efficacy. Its also clear that having too many guns around and letting them leak into places they shouldn’t be in, even if we have a good guy with a gun outside every school, is not effective in the sense of achieving what we want from guns which for the most part is Safety.
Seven
Targets are a bad idea. But if we can set a target for temperature rise, lets also Target:
- Turning around current falls in Life Expectancy.
- Stabilizing our Falling Replacement Rates
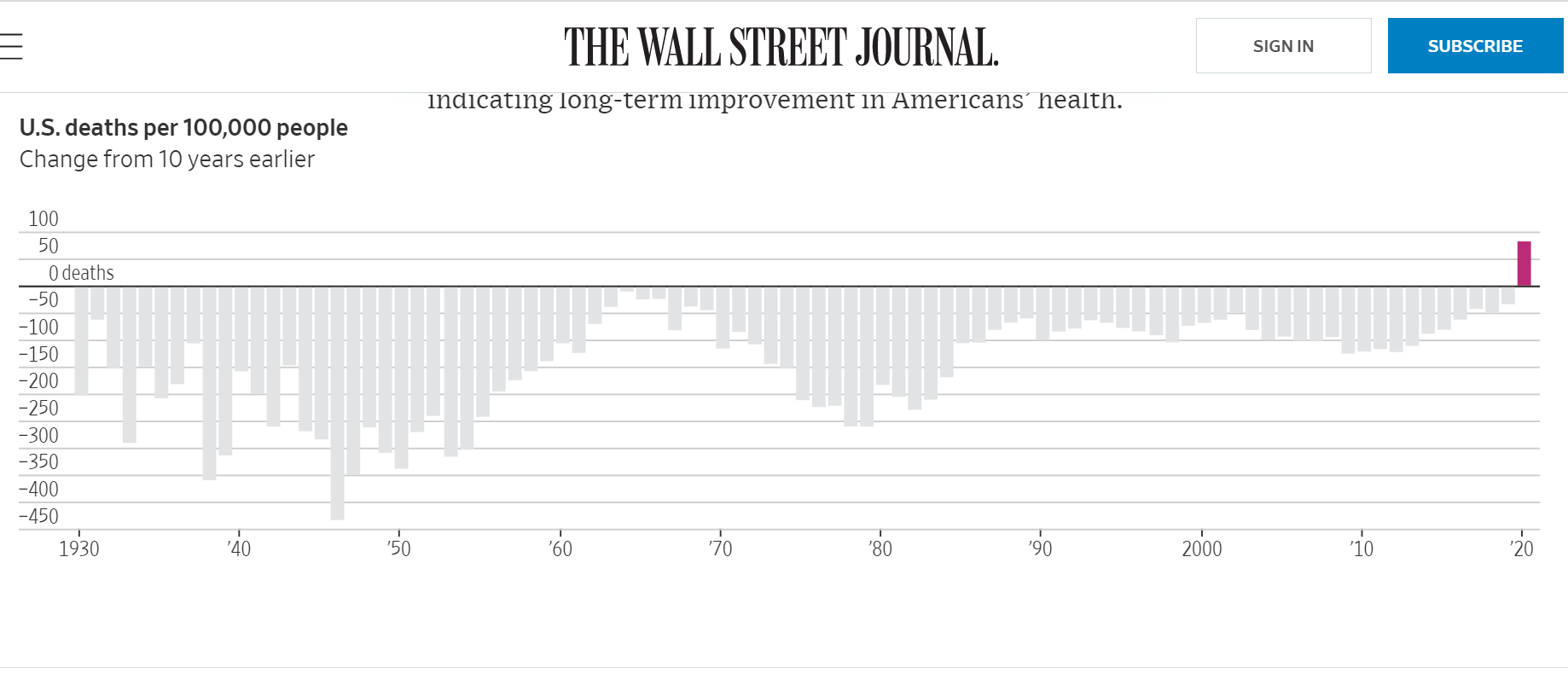
Re Life Expectancy, as this graph in the Wall Street Journal shows, with Covid we now have a dramatic fall in Life Expectancy.
Look not just at the red bar for 2020 but the ten years before that when life expectancy had been falling each year compared with ten years before that. The only comparable time this happened was in the 1950s and 1960s when the falling life expectancy was also put down to drugs – in this case tobacco.
The single easiest way to turn this trend around will be to deprescribe. There are now 3 studies looking at factors linked to Covid deaths and in all three the quantity of medication the person was on before they got ill has been a factor in their deaths – Dennis the Menace gets Covid.
Re Replacement Rates:

Across the Western World, roughly 15% of us take antidepressants. These affect the way every single one of us who takes them makes love, in most cases abolishing our ability and/or desire to do so, which of course affects another 15% of the population. This is increasingly a young person’s problems – not an old folks one.
(The BMJ article here blames depression but the kind of depression they are talking about increases sexual activity rather than reduces it and just as with the issue of Drugs and increased likelihood of death on Covid, journals are not happy to link any problems to the sacraments we are taking even when the problem is as obvious as genital numbing within the first 30 minutes after taking an antidepressant).
Given the uneven distribution of these drugs, it is quite likely there are areas of most countries where 20-30% of the population are not making love. At the moment, this is more a matter for white folk than for any other ethnic group.
If a woman does conceive, while on treatment, the meds double the rate of miscarriages, increase rates of voluntary terminations, double the rate of birth defects and double the rate of children who will have behavioural problems like autistic spectrum disorders. A recent estimate suggests a looming bill of over $5 trillion.
Eight
Drug regulation was based on Safety until 1962. A 1938 Safety Act in the United States kept thalidomide off the market there.
The Thalidomide tragedy triggered a change. Companies were required to prove the Efficacy of their drugs. This was supposed to contribute to Safety but this focus has given us weaker and weaker drugs with their hazards concealed – drugs are much less Safe now than they were in 1962.
Restoring the Primacy of Safety must be something for the first 100 days of office of any incoming administration that aims at Sustainable Healthcare.
In 1962, medicine was the scene of one of the strangest twists in human history. As of 1962, only one drug had ever been through a placebo and randomized controlled trial (RCT) before being brought on the market, in which it had been shown to be efficacious and safe – the test we now have in place to stop Thalidomide happening again.
That drug was Thalidomide.

Re Surveillance Capitalism ( UK is one of the most surveilled countries in the world.) There is still a month left for citizens to opt out of sharing all medical data – unless politicians and their networks are forced to extend the period again. Groups of doctors – Kudos to them – and others have carried out a huge campaign in UK to prevent them slipping it in under the radar There is still something missing Our data used for whatever purpose. should be made publicly available This site is intended for health professionals only
Meanwhile, figures show NHS Digital has recorded over three million national data opt-outs since 1 July 2021, from patients who do not want their confidential information to be used for anything other than their individual care.
NHS Digital launches data transparency tool as millions opt out of record sharing
NHS data
Caitlin Tilley (Pulse Today)
26 July 2021
Patients in England can now see which organisations have accessed their NHS data and for what purpose.
NHS Digital’s new Data Uses Register service intends to increase transparency around how patients’ data is used by third parties.
It comes as the Government was forced to delay the General Practice Data for Planning and Research (GPDPR) scheme again last week after a backlash over patient data safety.
Meanwhile, figures show NHS Digital has recorded over three million national data opt-outs since 1 July 2021, from patients who do not want their confidential information to be used for anything other than their individual care.
People can already see what data the NHS releases, but the new interactive tool allows people to see more clearly which institutions utilise the data, why they are allowed to access it and the anticipated benefits.
Organisations making use of the data include public sector bodies, charities or commercial organisations, who all legally have access for health and care-related planning and research.
Previous uses of the data include enhancing existing NHS patient services, creating new ones and assisting NHS organisations innovate new resources to offer better care.
The data can also help shape new treatments and aid NHS and local authorities with planning services.
For example, patient data was critical to determine which medications, including dexamethasone, were most successful for Covid patient outcomes in the University of Oxford’s Recovery trial. The drug went on to save more than a million lives worldwide.
NHS Digital’s interim chief executive Simon Bolton said the new Data Uses Register is ‘an important improvement to make our data sharing agreements more transparent and user-friendly’.
Beware of Everything – pot-shot at Horton
We have become used to the sight of politicians fighting like ferrets in a bag to ensure it is their rivals, and not they, who take the blame for any blunders in the battle against the coronavirus.
When, for unexplained reasons, it wouldn’t, he contacted Farrar, who reveals that he both emailed and texted The Lancet’s editor-in-chief, Dr Richard Horton — but got no response.
https://www.dailymail.co.uk/debate/article-9824485/DOMINIC-LAWSON-Scientists-adept-politicians-dodging-blame-coronavirus.html
It could have shattered the reputation of the entire advanced medical research profession globally. It would have been the scientists, and not the politicians (about whom Farrar is consistently critical in his book), charged with infamy and incompetence.
That would not have been a good thing, especially as it is British medical researchers, with Farrar’s involvement, who have done so much to improve the treatment of Covid-19.
But let’s not forget that the medical establishment has its own political prejudices, too: and it certainly seemed to prefer Beijing to the conspiracy theorist then in the White House.
‘free flow of critical ideas’ is beyond parody. …
More blah from the MHRA and Yet another independant group has been set up due to the need to protect the public somewhat from the regulators and their chums
PUBLISHED Yesterday at 08:00
This week the Department of Health and Social Care released the UK Government’s response to the recommendations of the Independent Medicines and Medical Devices Safety Review, sometimes referred to as the Cumberlege Review. In this blog Patient Safety Learning sets out its reflections on this.
Content
A year on from the publication of First Do No Harm, the report by the Independent Medicines and Medical Devices Safety (IMMDS) Review, the Government released its full response to the Review’s recommendations.[1] [2] Published alongside this was the report from the independent Patient Reference Group, established to provide advice, challenge and scrutiny to the work developing the Government’s response.[3]
Medicines and Healthcare products Regulatory Agency
The IMMDS Review highlighted several patient safety concerns relating to the role of the Medicines and Healthcare products Regulatory Agency (MHRA). It stated that the adverse event reporting and medical device regulation required significant revision and advised that the MHRA needed to ‘ensure that it engages more with patients and their outcomes’.[1]
The Government’s response fully accepts the Review’s recommendation calling for change at the MHRA. It then proceeds to outline a range of activities now being undertaken by the MHRA to improve its approach to patients, adverse event reporting and strengthening its regulatory approach.
Discussing the need for reform of the MHRA, the Patient Reference Group in its report noted:
The MHRA’s approach to patient engagement needs to become meaningful, to avoid being seen as simply a ‘tick box exercise’.[3]
Our reflections
We have recently responded to the MHRA directly with our patient safety reflections on one of the activities associated with the Government’s response, their proposed Patient and Public Involvement Strategy.[8] Our Chief Executive Helen Hughes has also provided comments directly to the MHRA as a member of the independent Patient Reference Group on their proposed Delivery Plan for 2021-2023 which is referenced in the Government’s response.[9]
The MHRA now has a stated ambition to become ‘a Patient focused regulator’.[10] Patient Safety Learning believes that achieving this will require more than just increased patient involvement, it will mean meeting patients’ expectations that healthcare products are safe, and patients are free from avoidable harm. Patient safety is not just about the safety of the product but its “safety in use”. There needs to be greater clarity about MHRA’s role and how it engages with the wider healthcare system to achieve this.
We also note that there has been a failure to acknowledge or address the serious criticism of the MHRA’s organisational culture in the IMMDS Review. Culture change is about more than staffing, governance, structures, and processes. It is also about leadership, behaviour, and psychological safety. There isn’t yet a clear picture of how the much-needed cultural change will be delivered. The MHRA has recently appointed a new Chief Safety Officer to support its work.[11] While this is a welcome development, there also needs to be explicit commitment to a focus on patient safety by the senior leadership of the MHRA; organisational culture is a Board and Executive leadership responsibility.
From a 2005 Report =the MHRA relies on company data, presented as a series of detailed assessment reports, in its decision whether or not to licence a drug. Raw data is very rarely analysed.
BRIEF
“I include the MHRA in my criticisms. When the public petitions committee took evidence from it, we learned that its detailed analysis amounted to three postgraduate students doing a desktop exercise for two weeks at a cost of £20,000 ($26,000),”
“The agency is not an effective watchdog. It does not take our concerns seriously. We have written to it a number of times and telephoned it, but we get standard copy-and-paste replies. The agency does not listen to us,” Holmes said.
Why should anybody trust this ……The Medicines and Healthcare products Regulatory Agency (MHRA) has created an Expert Working Group on Optimising Data on Medicines used During Pregnancy to ensure better data collection and analysis.
From Columbia Uni
Chile and Brazil are in the forefront of not just holding academic debates but thinking and doing something about the dangers of exploiting and damaging citizens inherent in the growing interest in neuroimaging and AI – (Not a squeak being heard of this in UK where neuroimaging research in mental health is well under way- Is there a Science Minister here?) Neuro rights are n fact regardless of new technigues ,being breached every day when drugs are prescribed designed to change brains One day doing things to peoples’ brains will possibly replace drugs – it is especially of interest to units already researching the brains of people diagnosed with ‘shizophrenia’ and in psychology circles ,the children being deemed as ‘inadequately’ parented- always vulnerable groups
NeuroRights Initiative
Technocratic Oath: Coming Soon
The NeuroRights Initiative, in collaboration with its partners, is drafting an ethical framework for entrepreneurs, physicians, and researchers developing Neurotechnology and AI called the Technocratic Oath.
Much as doctors must follow the Hippocratic oath, those who develop and administer neurotechnology would follow the “technocratic oath” The Five NeuroRights
The Right to Personal Identity: Boundaries must be developed to prohibit technology from disrupting the sense of self. When Neurotechnology connects individuals with digital networks, it could blur the line between a person’s consciousness and external technological inputs.
The Right to Free-Will: Individuals should have ultimate control over their own decision making, without unknown manipulation from external neurotechnologies.
The Right to Mental Privacy: Any data obtained from measuring neural activity (“NeuroData”) should be kept private.Moreover,thesale,commercialtransfer,anduseofneuraldatashouldbe strictly regulated.
The Right to Equal Access to Mental Augmentation: There should be established guidelines at both international and national levels regulating the development and applications of mental-enhancement neuro-technologies. These guidelines should be based on the principle of justice and guarantee equality of access to all citizens.
The Right to Protection from Algorithmic Bias: Countermeasures to combat bias should be the norm for machine learning. Algorithm design should include input from user groups to foundationally address bias.
Science Minister Couve (left), President Piñera (2ndfrom left), Professor Yuste (3rdfrom left) and Senator Giradi (right)
Science Minister Couve (left), President Piñera (2ndfrom left), Professor Yuste (3rdfrom left) and Senator Giradi (right)
Constitutional Amendment
NeuroProtection Bill
Technocratic Oath
Public Outreach
Brain-Computer Interfaces (BCI) Symposium
Data Handling and Security
Societal Impact and Regulation
congreso futuro
On the Necessity of Ethical Guidelines for Novel Neurotechnologies
PDF Download
Rafael Yuste Speech at the 140th Inter-Parliamentary Union Assembly (any one heard of an MP or AM or someone from college of psychs making any squeaks?)
PDF Download
Chilean Library of Congress Report on Neurotechnology
NeuroTechnologies: Connecting Human Brains to Computers and Related Ethical Challenges
The reason for needing the above
https://www.scielo.br/j/rbp/a/gQQPCpk4SXmH4znfZgftvSS/?lang=en
Eight
Restoring the Primacy of Safety
Stephen’s Voice – Suicide Prevention
@VoiceStephen
MISSD
@MISSDFoundation
Great to see Stephen’s Voice raising #PrescribedHarmAwareness. This letter to Ireland’s #health “leaders” is relevant to every country given serious adverse #drug effects and the lack of appropriate action from drug regulators & prescribers is a global problem.
https://twitter.com/VoiceStephen/status/1420343423786176514/photo/1
Current ‘Status’ …
https://www.dailymail.co.uk/money/markets/article-9836047/Glaxosmithkline-risks-losing-crown-worlds-biggest-vaccines-maker.html
Looks like the same loss of ‘Crown’ with Paxil/Seroxat – ‘lacked credibility’ – ‘deep expertise’ in pharmaceuticals –
‘left in the dust’ …