
This post, which opens with a photo of Noelia Voigt navigates between last week’s Cass and Cassandra, which features Distressed Damsels and Dudes, and RxISK’s post this week – Is Your Treatment Making you Suicidal, which features Dysphoric Damsels and Dudes – dying from drug induced dysphoria.
Noelia was until this week Miss USA 2023. She has stepped down from the post, citing a need to put her mental health first and hoping everyone tuning in will realise that even though stepping down from a role like Miss USA might make your future look very uncertain if you feel in your bones this is the right thing to do then be brave and do it.
Among the claims and counter-claims, there is one from a Noelia confidante claiming that Noelia was being silenced by the Miss USA organization – she could not advocate on social media for the issues that meant the most to her. Miss USA deny this claim.
Cheslie Kryst

Cheslie Kryst was Miss USA in 2019. She jumped off an upper floor of a New York skyscraper in 2022. She may have been depressed and on treatment for several years at least – a brief search through the first links that turn up don’t tell much.
Danny or David

David Blanchflower, more usually called Danny, is an economist who is very exercised by dramatic increases in rates of suicide among younger people especially women. The data below come from the United States but are paralleled in the UK and most other countries with no comparable increase in suicide rates in older ages.

The increased suicide rates are paralleled by increasing rates of despair among young women – teens and twenties – and young men – not found in older age groups/
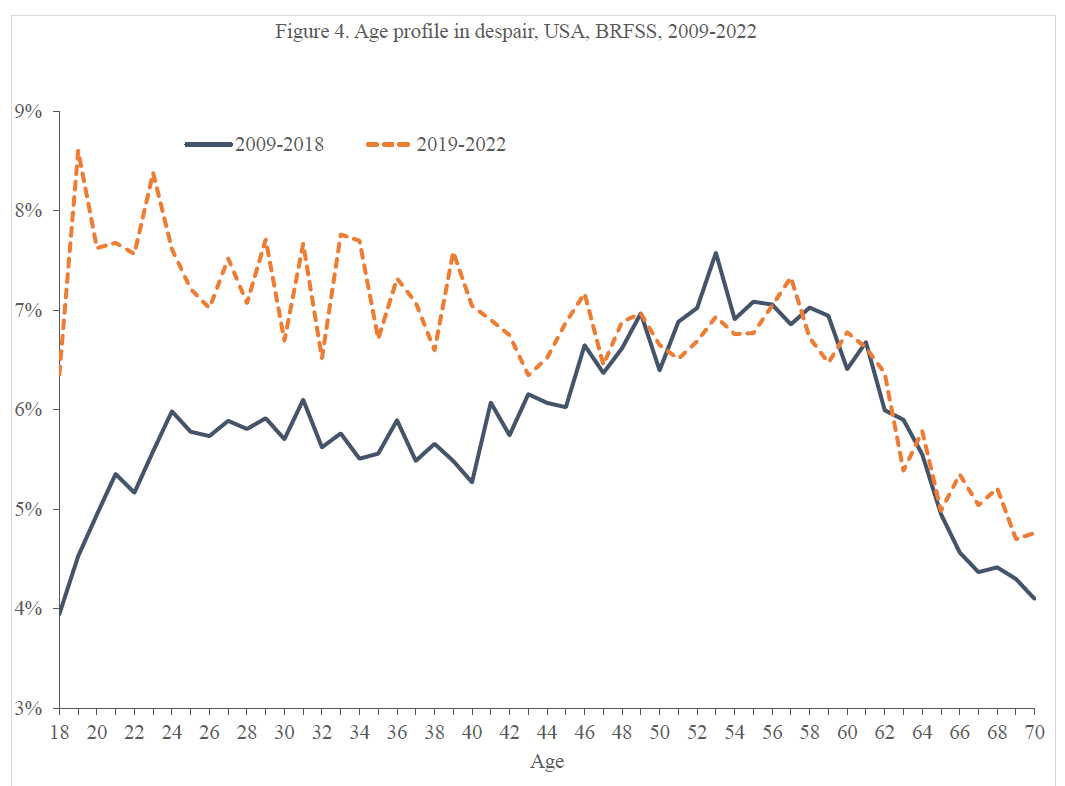
The blue line gives us as Blanchflower says one of the most established findings in all of the social sciences with 600 studies all saying the same thing – our middle years are the one’s where people are most stressed and unhappy and disabled. This established finding has had to be torn up in the last year or two in light of the red line which shows young folk now more disabled and despairing than any other age group.
The article from which these figures come is here – Blanchflower, Bryson and Xu. Danny has made several presentations based on the article, the most recent of which was in the U of Toronto a few days ago – The Declining Wellbeing of the Young.
The figures he shows map onto a graph that featured in The Great Silence – which shows a dramatic switch in young people claiming benefits – primarily for mental health reasons. They have diagnoses of ADHD and Autistic Spectrum Disorder but to be able to claim disability you have to not just have a diagnosis but to be able to persuade a panel of lawyers and doctors that you are unable to function.
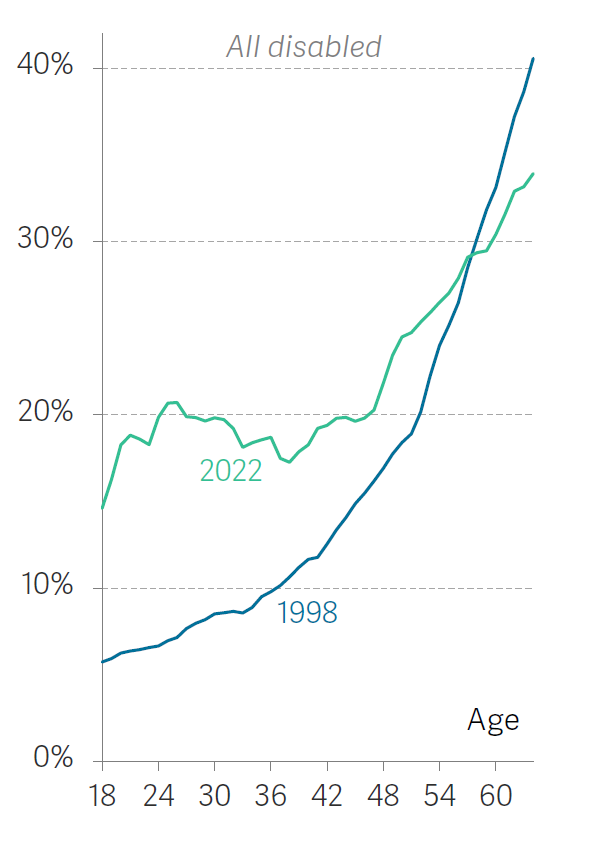
In the Great Silence, I mentioned that we don’t know where between 1998 and 2022 this switch happened – was it gradual or abrupt?
Social Media
Danny picks out 2011 as the year we began to see a difference. This was just after the first smartphones began to replace simple cellphones. Smartphones are everywhere in the world now, from Africa to America, and everywhere you see the same thing.
Simply having a smartphone in your hand doesn’t make you suicidal. Danny fingers the cyberbullying made possible by the phones as the trigger to suicide.
This fits into a growing narrative almost everywhere in the world. In the UK, the narrative can be traced back to the death of Molly Russell. The growing concerns were flagged up 5 years ago in Tinker, Tailor, Soldier, Surveillor as well as a first mention of the possibility that we might be making a significant mistake about what was causing the problem. It suited the Old Media to spin a New Media narrative.
This week the UK government have told the Big Social Media Companies that their Social Algorithms Must Change. The change isn’t going to be all that quick and it isn’t going to happen without pushback. Danny makes clear that he is facing the pushback lung cancer claimants faced – the so called evidence you are offering is just correlation not causation.
Cyberbullying
We can all agree that Social Media gives rise to some nasty stuff. Among the best examples are the ways in which doctors, especially psychiatrists, treat ‘patients’ on social media as this exchange between Nina and Dr Pinya Plomer illustrates.
This is mild compared to a lot of what happens. Anyone involved with the adverse effects of psychotropic drugs can easily generate a long list of much nastier stuff and can name the worst bullies – who are often well placed and even honored within their professional bodies in all ‘developed’ countries.

This Nina clearly stood her ground. She was the one doing the science. Unless you disbelieve her and everyone else who has been harmed, she is right to say she is the living proof of a harm and if Dr PP doesn’t engage with her, examine her record and her case, before shrieking – show me the proof – PP is just not being scientific. PP is gaslighting Nina and others.
Thanks to Harriet Vogt, who noticed this conversation and didn’t just forward it but jumped in.

Carl Elliott has an article in the New York Times this week about how Medicine Normalizes the Morally Unthinkable and creates a climate in which bullying not just can happen but is almost inevitable. For those of you, who like me, can’t afford to subscribe to the NYT and especially for those, who like me, figure the NYT and Guardian etc are at least as much and perhaps more to blame for these problems than Social Media, here is the Elliott Article.
Morally Unthinkable opens up with an example of medical students being more or less forced to examine the cervix of a woman who is under anesthesia. She has not been invited to consent to this before going under and is never told about it afterwards. What Morally Unthinkable does not tell you is that people like Dee Mangin were complaining about and putting a stop to this 40 years ago.
Bad practices can be stopped. It takes people to follow their gut instinct or the feeling in their bones – Juggling Selves and Bodies – as Noelia might say, or as was covered in Little Red Stethoscope nearly a decade ago.
The idea that damsels in distress might face more gaslighting and bullying from Old Media and Medicine than from social media does not appear at present to be on Danny’s radar.
Childhood
At the moment, Danny is liaising closely with Jonathan Haidt, whose recent The Anxious Generation is having quite an impact. T.A.G. covers issues Abigail Shrier covers in Bad Therapy but does so in a more balanced way.
Building on work by people like Peter Gray on children’s need for unsupervised play, The Anxious Generation picks out the denial of independence by droning parents and smartphones, which facilitate or create cyberbullying and droning, as giving rise to the problems we are now seeing.
There is something to be said for this. But who is anxious? Violence is almost by definition linked to Power. Those who have power have the means to be violent. Those without power may be episodically violent but do not have the means, or the drive or the organization to be systematically violent.
At present, those with power and money figure they’ve got to where they are by being rational – following the numbers, following the Science. As they see it, they can’t help it if they end up well-placed as a result – being irrational is not an answer.
An Us fractures into a Them and Us. We, who are uncomfortable with our wealth and power, start feeling they must be envious and plotting to take it away from us. Just to be safe, we need to gate our communities and drone our children – all of which become further markers of a violence and anticipatory rejection coming from the top down.
Old or New?
As laid out in Suicide: Are Old Media or New Media to Blame? and Tinker, Tailor, Surveillor, Facebook and Google have some easy responses.
We need to establish if it is their content that is causing the problem or if it is features like the Like and Dislike buttons that create in and out groups, that facilitate an apparent rejection by peers that is the bigger problem.
Just as removing weighing scales can do more to manage anorexia nervosa than any therapy or drug, so also removing the like buttons may do more to manage these new Neuroses than anything else could. See dashboard nervosa in Who’s Afraid of Science.
The social media companies are also in a great position to surveil people who may be trawling suicide or self-harm or distress sites. They can put early warning systems in place. This may conjure up a dystopian Minority Report scenario – but what are the old media or their allies doing?
The NYT, Guardian and related refuse to follow the data and the science.
- They will not report that the medical literature on on-patent drugs is ghostwritten to the point of claiming negative studies are positive.
- They facilitate the gaslighting of people or families who are harmed by reporting statements from professional bodies like APA or RCP stating that antidepressants save lives.
- This is a media service offered free to pharmaceutical companies by professional medical bodies – both denying the harms and wildly exaggerating the benefits.
- It cements in place medical perceptions that any warnings about drugs are the equivalent of May Contain Nuts labels on virtually every food product – efforts by companies and regulators to cover their back and so meaningless that even those with serious nut allergies pay no heed to them.
Whether you’ve been bullied on social media or not, even company trials show us that antidepressants cause more suicidal events than they prevent. In the case of healthy volunteers on them for a short time the rate can be up to 1 in 10 perfectly normal people becoming suicidal.
For some years Old Media mentioned things like this and it was possible to get articles in medical journals but for a decade before the first smartphone appeared, the Old Lay and Medical Media have been playing an intensely and increasingly active part in covering this up.
There is a lot of misleading information going around about the risks of antidepressants. The story some spin is that this in only a problem in younger people. Just the age groups Danny and Jonathan are talking about – without once it seems wondering if the drugs might be causing the problem.
This is wrong. The suicide event rate is as high in older groups. The difference is that the on average minimal benefit in groups of older people is just not there on average in groups of younger people. Which would be all the more reason to stop and think before using psychotropic drugs when someone arrives to a clinic in a state of distress having been cyberbullied by their peers or by health professionals or any state of distress.
Younger folk are much more likely to be distressed than they are to be mentally ill – this explains why it is so difficult to demonstrate the drugs work in younger age groups.
What a Big Phone You’ve Got Granny
All the better to treat you with my Dear.
So what should a doctor faced with a distressed young woman do? Distress is not a medical illness. Cyberbullying is distressing but SSRIs are no more an answer and perhaps not even as safe as telling her to turn to drink – our traditional bolt hole when a degree of emotional numbing is needed.
We can agree the increasing distress in young women from Greta Thunberg’s concerns for the environment to women with Rapid-Onset-Gender-Dysphoria must be something social. Smartphones are one possible trigger. But what about Moral Injury? See The Great Silence.
For over a century, since a communist revolution led by a woman, which Noelia may not realize was brutally put down, our social systems have turned to medical diagnoses like PTSD, as a means to divert the pressure from change away from changing the system and toward persuading the powerless the problems lie in them.
Carl Elliott says he used to figure it took bravery to speak out about abuses in medicine but changed his mind to figuring the system made sure physicians in training could no longer see a problem to get brave about. This misses the fact that young women, like Dee Mangin, did speak out about cervical examinations and changed the system. In most areas of medicine, the whistleblowers have been women.
Jonathan and Danny look like they want to be the woodman who rushes in to save Little Red – not realising there is no woodman in the original tales – see Little Red Stethoscope
Assuming they’d like to help rather than just be seen as Homo Ex Machina, should they focus on instances of social media cyberbullying or the fact that any doctor googling anything about drugs on their phone gets information from Old Media that denies there could be a problem with the meds and if Little Red seems worse this week than she was last week will hint at doubling the dose?
Women are probably braver than men when it comes to speaking out about things that count. By all accounts they have to deal with much more bullying all their lives than men and this was the case before smartphones. So why more suicides now? All thoughts on this would be good to get.
I find it impossible to tease out any one most significant the cause of more suicides or understand what the impact of prescription drugs could be. But it is interesting how many puzzled conversations older people are having about the number of youngsters being labelled with and wanting a mental health diagnosis especially ADHD and more so anxiety and depression which are seen as a cop out of dealing with life . I move around and hear it all over the place . Youngsters are cottoning onto the harms they can do but few mentions or warnings are being made anywhere of the potential harms even having a diagnosis can potentially be. Let’s not pretend the mentally ill tag is altogether acceptable and that it may potentially have worse consequences in harsher societies. There is no worthwhile employment; no affordable accommodation to rent or buy forcing people into unsuitable living conditions ;’and apply for stigmatised ‘benefits’; there is the way ‘they’ are talked about in derogatory terms’ the fear of what is happening world wide when no ‘adults seem able to deal with issues which are terrifying to anyone Is it it worth living in such a world or bringing children into it when prospects are so bleak is something I have heard ….Young People are being urged to aspire to much that is impossible or even desirable – there is a mantra in UK – if you can’t achieve you can end up working in a supermarket – where millions of people are doing just that valuable job and looked down on by media and politicians. Their elders cannot support them or do much to remedy things There are high rates of suicide in the countryside when conditions are no worse than they used to be. Homelessness in cities is massively increased .
A common factor is the interference in peoples lives by politicians so that choice and autonomy is undermined by more and more surveillance regulation and methods of undermining peoples’ control over significant parts of lives People on ‘benefits’ are being threatened once again by potential changes to the benefit system whereby doctors will lose the decision to write ‘sick notes’ – ‘specialists’ to be set up to decide and coerce people into often unsuitable employment. Youngsters of the well off are not subjected to this It is a significant division of the them and us. This policy tried and dropped before led to a lot of suicides. A factor that stands out for me is that there is more coercive harmful control over peoples’ lives than there used to be
Just by the way re the intimate examination of womens’ bodies. It may have been stopped over 30 years ago in Canada but was still happening in UK much later. I found out I had been examined by a bunch of students under anaesthetic and it had been photographed . The last thing I saw when being given the anaesthetic was a camera above the bed. I reported this and was told the surgeon had said it was normal procedure . Luckily the person I referred it to understood it was an unacceptable violation that it was embarrassing to complain so who knows how many women had been violated . He eventually agreed it was wrong as he must have known all along as it was done secretly and the manager had a consent policy put in place. We are not just bodies we are human beings. A fact which applies to what I am trying to say above as well.
So why more suicides now?
‘The question is whether this rise in mental illness in the young is a permanent or temporary change and if this change in the relationship between age and well-being has occurred in other countries. The big question then is what to do about it?
That is the subject of our ongoing research.’ – David G. Blanchflower Alex Bryson Xiaowei Xu
This was also covered in a Programme last night –
Happiness is U-shaped
https://www.bbc.co.uk/programmes/m001r2wr
Middle age is a time of great disappointment, you are not going to win a nobel prize, you won’t become CEO of a company, your aspirations are not like those you had in your youth – to paraphrase.
Good for Harriet, calling out the bullying, I did not find my doctors to be gentle, sympathetically-inclined, ‘pillars of the establishment’, or remotely knowledgeable about antidepressants, or benzos, or beta-blockers, or, even ‘suicide’.
‘in general incompetent’
Being prescribed to any age, is fraught with danger.
My doctor was a Guardian reader. The Best and the Most Well-Informed was Sarah Boseley of The Guardian. As I would bang on about Seroxat, sitting in her garden on an Island, she would never, ever respond. She would sit with her newspaper, half-pretending to listen. It would take an epic loss of concentration to avoid the amount of Boseley articles centering on GlaxoSmithKline and Seroxat.
‘its reporters and editors are, in general, incompetent’
Not really. They have been brain-washed and bullied by Pharmaceutical Companies, and Medical Journals, where the absolute truth is missing in action – the ghostwriters.
‘Red-Herrings’ all over the place; it is a massive struggle to find the truth, and if we can’t find it, who will?
U-shaped; U-shape…
Why is Happiness U shaped? Bizarre.
Youth suicides and supposedly more girls. Girls are being drugged for ADHD. Big Pharma discovered this untapped niche a while back!
Youth suicides +++. Children need their mothers, fathers, parents. Over the past three to five decades parents have increasingly used non-parental care and children have been commodified.
Youth suicides +++. Lack of family supports, extended family, and healthy finances.
Youth suicides +++. Education that is discriminatory and highly competitive with schools and institutions and teachers and educators focusing on the best and rewarding the best.
Poor classroom skills allow for scapegoating of non-compliant children heading them and their families down paths of psychological assessments, psychiatric drugs, and of course the all important extra financial funding given to schools.
Youth suicides +++. Resources being made available selectively and given to the most promising of students.
The list could go on … but you have the general idea.
We are a society that offers troubled young people, in lieu of meaningful help, pills known to cause worsening depression and suicidality. Then, when they become depressed and suicidal, instead of taking them off the drugs, we offer them assisted suicide.
https://www.bbc.com/news/stories-45117163
https://www.youtube.com/watch?v=SWWkUzkfJ4M&rco=1
https://www.youtube.com/watch?v=6QJMrEvKwmI
https://www.youtube.com/watch?v=7-w6c-ybwXk
https://www.youtube.com/watch?v=cMeub1Gkjnw
https://www.baltimoresun.com/author/patrick-d-hahn/
We have become a society devouring its own children.
I agree that both Smartphones and SSRI’s are contributing to the avalanche of mental-health distress in youth. And there may be interactions that doctors fail to recognize.
While D. Blanchflower is right that cyber-bullying is a huge problem, there are other toxic effects of “growing up online.” One is the social-comparison effect of being bombarded with content from peers (both friends and strangers) whose perfect looks and awesome lifestyles make you feel like a loser. It’s exacerbated by the need to curate your own self-display, then wait anxiously for “likes.” This hits hardest at girls, but boys can also fall victim. Some kids also fail to develop the skills that come from real-time, face-to-face interactions. Like patching up quarrels, dealing with bullies and Mean Girls, or asking for a date.
Another is the algorithms designed to maximize ad revenue by serving up more and higher doses of the stuff you seem to like (as with poor Molly Russell, whose parents found loads of disturbing videos about cutting and suicide on her phone after her suicide). Kids who click on a bit of self-harm or pro-anorexia content can get flooded with more of the same. This can produce compulsive behavior in people with no history of OCD—in fact it’s designed to do so. The phrase “falling down the rabbit-hole” is used these days by people of all ages to describe a new obsession with some topic or other, which usually begins online.
Doctors and LPNs trained to screen everyone for depression, anxiety, OCD, PTSD etc. can easily overlook the role of the online environment where a kid hangs out – and react with a diagnosis and prescription. For lots of kids, this predictably makes the situation worse. Especially if the drug produces “disinhibition” which leads to risky or impulsive behavior, including suicide.
Very astute analysis, Johanna.
Ofc cyberbullying is a scourge. Having your psyche torn apart, not by a few mean kids, but by an unknown army of sneering people in front of a global audience. That seems to have been what destroyed Cheslie Kryst – although there’s a lot of press comment about her unmedicated ‘high functioning depression’ – a set of words without meaning for me.
I also wonder if there’s another explanatory dimension – a tendency amongst Zoomers living in cyberspace to be disconnected or alienated from their whole, integrated selves.? Perhaps an obvious thought, but Danny doesn’t seem to have had it.
When young people are, as you say, curating (perfect 21st century word) their identities for display purposes, like brands on a virtual shelf. Assembling their identities from pick ‘n mix sexual orientation labels more than real world sexual pleasure, their looks through filters, their emotions from extrinsically imposed diagnoses – and then, maybe top it all off by swallowing an emotionally constricting drug. It’s dystopian.
Are there cases when some of these Zoomers just don’t fully connect with the reality of death, being no more? At some level, do they feel they are discarding a surface, sort of stuck on identity, rather than extinguishing living flesh and blood?
It’s a genuine question. I’ve certainly seen people so emotionally constricted by antidepressants – ‘zombie’ was the word Kristina Kaiser used to describe her beautiful daughter Natalie’s iatrogenic state. How clearly can a person reduced to that extreme of emotional absence feel about the value of being alive? Especially if their self is an identity confection?
Speaking of the NYT, there has been a recent article in the NYT called What You Really Need to Know About Antidepressants. Very demoralising…
‘Social Intervention’ Sounds benign but predictably coercive .People in vulnerable economic situations will be the greater target for interventions .Critics are rightly asking whether doctors should be meddling in peoples’ private social lives. If the consequence of not accepting social prescriptions will be loss of income then suicides will happen as proven when coercive employment strategies have been tried. Sir/Dr Sam Etherington the lead promoter of this policy in UK constantly says that his aim is to get people of ‘sickness benefit and into work – Sam knows this is good for them instead of ‘sitting all day watching a flickering TV screen’.
Shifting the Balance Towards Social Intervention: why the UN and WHO are calling for mental health reform
IIPDW
Shifting the balance towards social interventions: why the UN and WHO are calling for mental health reform
Nearly a quarter of the adult population is prescribed a psychiatric drug every year, and a similar proportion of young people meet the criteria for a mental health diagnosis.
The situation is worsening every year – but despite billions of pounds of investment, mental health outcomes are no better than 40 years ago and psychiatric drug efficacy has not improved.
There has to be a better way.
The UK’s Beyond Pills All-Party Parliamentary Group is hosting an online seminar on Tuesday to launch a new report ‘Shifting the Balance Towards Social Interventions: a Call for an Overhaul of the Mental Health System’. The event will be hosted by Lord Crisp, former chief executive of NHS England, and include contributions from:
– Dainius Pūras, the former United Nations (UN) Human Rights Council’s Special Rapporteur
– Michelle Funk, Unit Head of the WHO Policy, Law and Human Rights team
– Sir Norman Lamb, Chair of the South London and Maudsley NHS Foundation Trust
This highly informative and timely webinar will hear key messages from UN and WHO reports and consider what steps the UK should be taking to reform its approach to mental health prevention and treatment.
Please register soon for this invitation-only event which will take place online on May 14th from 11-12:30 BST. You will need to use your Zoom account to register – one can be created free of charge if you don’t already have one.
Any queries about registration please send to admin@beyondpillsappg.org.
Prozac one of 30 antidepressants probed by UK watchdog over links to suicide
https://www.independent.co.uk/news/health/antidepressants-prozac-suicide-rates-side-effects-b2542357.html
More than 30 of the most common antidepressants used in the UK are to be reviewed by the UK’s medicines regulator, as figures point to hundreds of deaths linked to suicide and self-harm among people prescribed these drugs.
The medicines, which include Prozac and are prescribed to millions of patients, will all be looked at by the Medicines and Healthcare products Regulatory Agency (MHRA).
It follows concerns raised by families in Britain over the adequacy of safety measures in place to protect those taking the drugs, such as warnings about potential side effects.
The regulator will look into the effectiveness of the current warnings, according to a letter from mental health minister Maria Caulfield, which has been seen by The Independent.
There has been a huge rise in the use of antidepressants in England, with 85 million prescriptions issued in 2022-23, up from 58 million in 2015-16, according to NHS figures.
Nigel Crisp, a crossbench peer and chair of the Beyond Pills all-party parliamentary group, told The Independent: “Overprescribing of antidepressants has an enormous cost in terms of human suffering, because so many people become dependent and then struggle to get off them – and it wastes vital NHS resources.”
The review comes as it emerged that:
More than 515 death alerts linked to these drugs, involving suicidal ideation and self-harm, have been made to the MHRA since the year 2000 (these alerts don’t directly confirm the cause of a person’s death)
Side effects of many antidepressants can include suicidal thoughts and anxiety, according to the National Institute for Health and Care Excellence (NICE), though this is considered uncommon
Some antidepressants have been given to children as young as four, and the total cost of the medication to the NHS in 2022-23 was more than £231 million
One mother, Lyn Richardson, called on the regulator via The Independent to review safety measures around the drug mirtazapine after her daughter took her own life two weeks after being prescribed it.
The regulator confirmed to The Independent that the expert working group will look at 30 different medications. Drugs include fluoxetine, the brand name of which is Prozac, lithium, and citalopram.
According to MHRA data, fluoxetine has prompted 9,237 serious and fatal alerts over adverse reactions since 2000 . Of those, 438 were related to “suicidal and self-injurious behaviours” and 286 were linked to anxiety symptoms.
Data suggests there have been 73 fatalities linked to suicidal and self-injurious behaviours in the last two decades. The data does not confirm the drugs are a direct cause of death.
Last week The Independent reported on calls from Ms Richardson for the regulator to review safety measures around mirtazapine after her daughter Rebecca Kruza took her own life two weeks after being prescribed the medication.
Mirtazapine, which was given a “black box” alert in the USA due to its side effects, has had 59 alerts linked to suicidal and self-injurious behaviours. This led to the US regulator placing clearer warnings on the packaging.
It will be included in the MHRA’s wider review.
In a letter to Ms Richardson, Ms Caulfield said the MHRA’s review will look into the effectiveness of the warnings about suicide relating to antidepressants.
As the use of antidepressants soars, the most recent NHS data from March 2023 to December 2023 shows 331,000 10 to 19 year olds were prescribed an antidepressant – up from 240,000 during the same period in 2015-16.
Last year, the Beyond Pills APPG called for government action to reverse the increase in prescriptions of these drugs.
Professor James Davies, associate professor of Psychology at University of Roehampton and member of the Beyond Pills APPG, warned there were “insufficient” provision of social and psychological alternatives to medication.
While 8.5 million people were prescribed anti-depressants in 2022-23, only 1.2 million people started talking threapy treatment.
“We have over 85 million prescriptions of these drugs each year in England, and that figure grows yearly,” he said.
“Another concern is not only are we seeing vaulted rates of prescribing to the general population, we’re seeing the average duration of time a given person spends on these drugs increasing as well…
“One of the reasons for this is that there’s still insufficient provision for social and psychological alternatives in the NHS.”
He warned patients are not being adequately followed up once they have been prescribed these medications.
Professor Davies added: “We should not be prescribing these psychotropics to young people. We should be providing young people with the psychological and social support necessary to enable them to overcome the difficulties that they’re encountering.”
The MHRA said it could not confirm the scope of the review or what actions could be taken as a result as it was still convening its panel of experts.
It told The Independent: “We are currently finalising the core membership of the expert working group considering risk minimisation measures for antidepressants and anticipate that their first meeting will take place in July. The group will be considering all antidepressants on the UK market.”
Professor Davies highlighted concerns over the regulator’s ability to conduct the review.
He said: “The MHRA is far too close with the industry to be objective for this review, in my view. It is 100 per cent funded by the pharmaceutical industry. There are serious concerns about what we call regulatory capture which is when it is far too close to the industry it is purporting to independently regulate.”
An MHRA spokesperson said it had “robust conflict of interest mechanisms covering MHRA staff, board members and those who give independent, expert advice on MHRA committees. These mitigate any potential conflicts of interest effectively”.
Dr Amit Aggarwal, from the Association of the British Pharmaceutical Industry (ABPI), said companies support “ethical and evidence-based prescribing”, and wants to help healthcare professionals and patients reach sensible decisions on best treatment.
A Department of Health and Social Care spokesperson said Talking Therapies was the recommended first line treatment and that the scheme is expanding to include 384,000 more people over the next five years.
It added: “The decision to prescribe a particular product is a clinical one and should be based on the patient’s medical need, taking into account NICE guidelines, which recommend not routinely offering antidepressant medication as a first-line treatment for less severe depression.”
Eli Lilly, which owns Prozac, told The Independent: “There is nothing more important to Lilly than the safety of our medicines. For decades, Lilly has been submitting fluoxetine safety data, to regulatory authorities around the world, including the MHRA and FDA.
“Fluoxetine is approved by the MHRA and FDA and continues to be considered to have a positive benefit-risk profile by regulatory authorities, physicians and patients around the world.”
32 comments published which will be worth reading and adding to in the Independent Article
This makes Katinka’s Petition of even greater importance.
The avoidable suicide tragedies are only a part of this antidepressant prescription drug catastrophe.
Those who developed AKATHISIA, EMOTIONAL BLUNTING and DISINHIBITION as a result of being inappropriately coerced by prescribers into taking SSRI/SNRI/’Atypical ADs, and then had Adverse Drug Reactions (ADRs) and withdrawal syndromes repeatedly misdiagnosed as Serious Mental Illness, have had their lives destroyed.
Their families suffer and struggle 24/7 with multi-systems. lifelong injuries in their loved ones. They live with iatrogenic disability denied by prescribers.
The potential to receive desperately needed State Benefits is denied by the refusal of medical practitioners to endorse expert reports that they have never had a Mental Illness,
Refusal to confirm that they have entirely prescription drug-induced life destruction: – (Intensified by multiple psychiatric misdiagnosis, inappropriate serial incarceration, enforced further psychotropic drug injuries and labels for life which exclude them from mainstream society). ISOLATED. LONELY. REJECTED.
Where is the reference to the fact that these drugs are far more powerful anti-libidinous chemicals than ‘effective antidepressants’? Will their use in the ‘chemical castration’ of ‘volunteer’, convicted sex offenders be considered.
Are we going to have an accurate and trustworthy identification of Conflicts of Interest in the MHRA’s ‘Expert’ Committee?
Will this exercise identify the multitude of those so badly injured by these drugs that they are excluded from the work-force: – “Economically Inactive”! – because they were ill-advised enough accept their doctor’s advice to take ADs for normal life adversity? Drugged and damaged without Fair, Full and Informed Consent.
Might in be high time to REGULATE THE REGULATORS?
Tim Peter Doshi refers to the FDA but shows why the answer to your question ‘Are we going to have an accurate and trustworthy identification of Conflicts of Interest in the MHRA’s ‘Expert’ Committee?’ is unlikely.
BMJ Investigation
Revolving doors: board memberships, hedge funds, and the FDA chiefs responsible for regulating industry
BMJ 2024; 385 doi: https://doi.org/10.1136/bmj.q975 (Published 08 May 2024)
Cite this as: BMJ 2024;385:q975
Peter Doshi, senior editor
The US Food and Drug Administration says that it takes conflicts of interest seriously. But financial entanglements with the drug industry are common among its leaders. Peter Doshi reports
At his public confirmation hearing in late 2021, Robert Califf, President Biden’s nominee to lead the US Food and Drug Administration (FDA), faced pointed questions about his financial relationships with industry.
Bernie Sanders, the senator from Vermont, asked, “At a time when the American people are outraged by the high cost of prescription drugs, deeply disturbed about what happened with Purdue and Oxycontin, what kind of comfort can you give to the American people when you have been so closely tied to the pharmaceutical industry yourself?” He added, “How can the American people feel comfortable you’re going to stand up to this powerful special interest?” Califf responded: “Senator Sanders, I have a history of doing that. But I’d also point out that this administration has the most stringent ethics pledge in the history of administrations.”
Califf did not earn Sanders’s vote, but he got the job. With it, the incoming FDA commissioner committed to sell his pharmaceutical stocks and sever his financial relationships with biotech companies such as Alphabet owned Verily Life Sciences, which paid Califf $2.7m as a senior adviser, according to his federal disclosure (see supplementary files on bmj.com).
The divestitures were not the product of an ethics pledge, nor were they optional. Criminal conflict of interest rules prohibit government employees from “participating personally and substantially in official matters where they have a financial interest.”1 Other regulations prohibit FDA employees from holding financial interests in any FDA “significantly regulated organisation” such as drug and medical device companies.2
Failure to comply can be costly. In 2007, a former FDA commissioner—Lester Crawford—was sentenced to three years of supervised probation and fined $89 377 for false reports about stocks that he and his wife owned in four FDA regulated companies.3 Crawford, a pharmacologist and veterinarian who had served in the agency on multiple occasions before being nominated as commissioner, had been instructed to sell stocks in around a dozen regulated companies. But he did not sell shares in three of these companies:
The year 2022 marked Califf’s second time leading the FDA, having previously served during the Obama administration’s final year. It was therefore his second time terminating a host of ties with the companies that the agency is meant to regulate, and his second time signing an ethics pledge.
The Trump administration, too, required that appointees sign an ethics pledge, committing not to lobby the agencies for five years after public service. But the requirement was rescinded on 19 January 2020, Trump’s last full day in office. In addition, the ban only applied to lobbying activities, not employment in general, and within three months of vacating the FDA’s top job, Scott Gottlieb, Trump’s first nominee who led the agency from 2017 to 2019, was nominated to Pfizer’s board of directors, subsequently gaining enormous public visibility through regular media appearances as a covid expert commentator. (While a medical student, Gottlieb interned at The BMJ as a Clegg scholar; he subsequently penned a number of BMJ news articles.)
The revolving door between the FDA and industry surprises few anymore, despite the widely acknowledged potential it has for undermining public trust in government. And stories about FDA commissioners’ heavy ties to industry have become commonplace: nine of the FDA’s past 10 commissioners went on to work for the drug industry or serve on the board of directors of a drug company.
But the story of Margaret Hamburg, Califf’s predecessor who led the FDA between 2009 and 2015, is less well known, apart from coverage in local press.5 Like her colleagues, Hamburg had relationships with FDA regulated companies before and after her stint at the FDA’s helm. But unlike her colleagues, Hamburg was allowed to hold financial interests in an exclusive hedge fund managed by her husband’s company.6 And in an analysis conducted by The BMJ (see table), the hedge fund consistently invested in FDA regulated drug companies during Hamburg’s time at the FDA.
RenTec
The hedge fund, Renaissance Technologies, is one of the biggest and most profitable companies of its kind. It is also one of the most secretive and exclusive. Renaissance pioneered “quantitative trading,” the use of statistical models to drive high frequency stock trading decisions, and became what some have called “the greatest modern day moneymaker,”7 with almost mythic status in the business community. Its flagship product, the Medallion Fund, has averaged annual gains of 39% after fees over three decades,8 earning billions for its investors. But the lucrative fund is reportedly only open to the firm’s employees, their families, and select friends.9
Hamburg was one of those fortunate investors, thanks to her husband Peter Brown, a senior employee at Renaissance. In 2010, the year after Hamburg was sworn in as the new head of food and drugs, Brown became Renaissance Technologies’ co-chief executive officer, and in 2012, with $125m in earnings, was rated by Forbes Magazine as the 16th highest earning hedge fund manager.10
FDA policy—then and now—states that “FDA employees are prohibited from holding interests in certain investment funds that have a stated policy or practice of investing in companies that are SROs [significantly regulated organisations].”11 And the law attributes the interests of spouses to the government employee.1 An independent agency known as the Office of Government Ethics (OGE) reviews the financial disclosures of senior executive branch nominees to identify potential conflicts of interest.
Following the OGE’s review and before becoming FDA commissioner, Hamburg pledged to resign from more than 10 non-profit organisations at which she held a senior position and from the board of Henry Schein, a massive healthcare products supplier company. Brown sold his stock in Johnson & Johnson and Merck, among others, and the couple divested from several fund holdings at Renaissance. But they were both allowed to keep their holdings in the Medallion Fund which, according to financial declarations, earned them more than $3m between 2009 and 2010. Brown kept his job at Renaissance, which shares its profits with employees, and apart from Medallion Fund income, he reported payments from Renaissance between 2008 and 2010 in excess of $1m each year. (The actual amounts earned while Hamburg led the FDA might be much larger as The BMJ only reviewed forms for Hamburg’s first two years as commissioner, and spouses are not required to report in any specificity beyond “over $1 000 000.”)
Why the OGE permitted these arrangements is unclear. The OGE does not make its deliberations public and, in response to a request from The BMJ, the office said that it “does not respond to questions about specific individuals.”
The FDA also declined to provide any specifics of its evaluation of Hamburg’s relationships with Renaissance. In an emailed statement, a spokesperson stated: “As part of the confirmation process, Dr Hamburg—like all FDA commissioners—underwent rigorous pre-approval and clearance procedures including review by the US Department of Health and Human Services Office of General Counsel Ethics Division, the US Office of Government Ethics, and the US Senate. Any potential conflicts were resolved with those entities prior to her confirmation.”
According to an unnamed “administration official” who spoke to the Wall Street Journal in 2009, the couple were allowed to retain their holdings in Medallion because the fund is based on programming that “does not allow for human tracking or input except in rare instances,” and trades rapidly, holding shares only briefly, “meaning that neither Dr Hamburg nor her husband would be in a position to direct their Medallion account to companies or areas affected by the FDA.”6
Richard Painter, a professor of corporate law at the University of Minnesota and former chief ethics lawyer for President George W Bush, although not familiar with the details of Renaissance or Hamburg, commented that a lack of human involvement in Medallion might at least partially address the potential for insider trading, which can be criminally prosecuted as a felony. “If the computer’s making the trades, I’m not too worried about government information getting into the company. I’m not as worried about the insider trading problem.”
But the degree to which the algorithm controlling Medallion actually operated without human input was called into question by a 2014 Senate investigation into the abuse of structured financial products. In July 2014, the investigation’s chairman, Senator Carl Levin questioned Brown, who was co-chief executive officer of Renaissance Technologies at the time.
Levin asked Brown: “You make it sound like the selections were made by a machine with no human intervention. Now, your scientists and your experts are continually looking for inefficiencies in the market, and when they find something new . . . they try to adjust the computer model and incorporate that into the algorithm, and that will affect the decisions that are generated. It could also have an impact on what positions are bought and sold. So there is a lot of ongoing human involvement in this process. Is that correct?”1213
“That is correct,” Brown responded.
Levin continued for eight minutes, identifying the number of employees involved in making those changes and the frequency of changes: “This algorithm wasn’t just making changes by itself. It took human beings to make changes.”
Brown: “Yeah sure, the human beings wrote the code.”
Levin: “Good. And changed the code?”
Brown: “That’s correct.”
Levin: “Tweaked the code and once or twice every week changed . . . ”
Brown: “On average.”
The Senate report summarised the matter: “According to RenTec [Renaissance Technologies], its trading algorithms were dynamic and had to be updated and adjusted on a regular basis by its programmers. RenTec explained that the algorithm was frequently modified manually by programmers”—modifications that could be used “to direct trades to particular options to reduce or increase its portfolio size.”14
The BMJ asked Brown to explain the discrepancy between his Congressional testimony indicating that RenTec employees regularly intervened in the algorithm and statements elsewhere that there was “no human intervention except in rare circumstances.” But he did not respond to a request to be interviewed for this article, and his spokesperson, Jonathan Gasthalter, would only speak off the record.
High frequency trading with a proprietary algorithm partly explains why the Medallion Fund has been dubbed the “blackest box in all of finance.” What, precisely, it is invested in, for how long, and how much are ever changing and unknown. But what is known is the overall holdings of the company and that the Medallion Fund is far and away the company’s crown jewel.
Thanks to disclosure requirements, companies like Renaissance file quarterly reports with the Securities and Exchange Commission, which publicly posts them on its website. And a review by The BMJ found that, in every quarterly disclosure for the past 20 years, including the six in which Hamburg served as FDA commissioner, Renaissance Technologies held stock in FDA regulated companies. In all 24 of the quarterly reports filed during Hamburg’s tenure at FDA, Renaissance held stock in three major drug companies—Amgen, Novo Nordisk, and AstraZeneca—at an average value of $518m. Across 10 drug companies, the reports indicate average holdings of over $1bn (table).
The facts raise concerns over the adequacy of current rules governing financial holdings by FDA commissioners.
“This is something the OGE should have shut down right away,” says Craig Holman, a government affairs lobbyist for the consumer advocacy organisation Public Citizen, who was not familiar with the details of Hamburg’s case. “I’ve got a feeling they just didn’t quite understand how these algorithms work—and were just inexperienced.” He adds: “The OGE usually is quite good at moderating and mitigating conflicts of interest among the executive branch . . . I’ve always had quite a bit of respect for them.”
Hamburg declined an interview request from The BMJ, but in response to questions about her private conversations with the OGE, emailed a response through her personal communications agent: “In my capacity as a physician and a government official, I have always taken my ethical obligations very seriously. Prior to my confirmation as FDA commissioner, the US Senate and the Office of Government Ethics (OGE) thoroughly evaluated any potential conflicts, including those that might arise as a result of my husband’s position. Those potential conflicts were addressed in signed ethics agreements, and submitted financial disclosure reports were reviewed annually by the OGE during my tenure as commissioner.”
Painter thinks that the OGE is mostly focused on assessing whether there is anything a government employee could do in their official position that would have a “direct and predictable effect” on their (or their spouse’s) investments or salary. Although preventing such conflicts of interest is essential, Painter says that better protections against insider trading on government information are also urgently needed, something the OGE “has relatively little expertise in dealing with.”
“Government leaks like a sieve,” he adds, with routine unauthorised disclosure of non-public government information. Although RenTec’s headquarters are in New York, “you have got a lot of hedge funds operating out of [Washington] DC, and I know exactly why they’re there. They’re trying to get non-public information out of the government.”
In Holman’s view, the OGE must be strengthened. Currently, the agency is small, with around 70 employees, and is focused on issuing advice, for example about divestiture, with limited ability to enforce its recommendations. In 2021, Holman helped draft legislation, introduced by Senator Richard Blumenthal of Connecticut, aimed at turning the OGE “into an actual ethics cop with enforcement authority and much greater transparency.”15
Today Blumenthal leads the Senate Permanent Subcommittee on Investigations, the same panel that, 10 years ago, under Levin’s leadership, investigated Renaissance Technologies, and concluded that Renaissance Technologies had avoided more than $6bn in taxes.
After fighting the tax evasion charge for years, in September 2021, Brown informed Medallion Fund investors that Renaissance had “resolved our longstanding dispute” with the government.16 Current and former investors would be required to pay, with Renaissance’s seven board members during 2005-15 and their spouses “being subject to substantially more costly terms.” The total cost of the settlement was not given but was reported in the press as up to $7bn.17
Brown and Hamburg did not respond to The BMJ’s query regarding how much of this penalty they are paying.
Table Renaissance Technologies’ holdings in 10 selected drug companies reported in ≥75% of quarterly public disclosure reports while Hamburg was FDA commissioner
View popupView inline
For a smart and nuanced guy, Peter has a touching but difficult to understand faith in bureaucrats. FDA, EMA and MHRA and their conflicts of interest are semi-irrelevant. The missing in action guys are the medical profession who need some conflicts of interest – they need to realise that if drugs have no harms doctors are going out of business.
D
Susanne, Thank you for addressing my concerns about an “Accurate and trustworthy identification of conflicts of interest by medical regulators”.
This doesn’t appear to be a priority on reading your very detailed response above!
Failed regulation leads to avoidable injury, avoidable deaths and destroyed lives.
It seems that those who prescribe may be naive in their trust in drug and appliance approval and licensing?
Tim – Susanne
There is a mystery here. FDA regulate tobacco as well as drugs and I expect alcohol also. But when things go wrong with either of those we don’t think about complaining about regulators or suing them – we sue the companies that make them. Ditto automobiles and every other consumer product.
Why on earth do you think its a failure of regulation when things go wrong on drugs? It isn’t. There are 2 groups failing us – companies and doctors. Regulators are a bunch of bureaucrats who know nothing about clinical practice. Even the GMC who do regulate Medical Practice stick to gross breaches of conduct like taking sexual advantage of people – they do not take a view about clinical practice that kills and injures people. That’s up to doctors to sort out and us to sue them if we have to.
It suits doctors and companies that you both – and Peter Doshi and I guess BMJ – finger regulators. You keep them laughing all the way to wherever they go to figure you can fool all the people all the time
David
I do admire the commitment of Petr Doshi who is using the funds provided by Thebmj to highlight issues like this. Why on earth shouldn’t I take his investigation(s) seriously
I don’t think any of us are pointing the finger only at regulators Most of us understand there is a network involved in the failings to protect from harm. They are the focus of the article though. That they are a massive problem is undeniable surely they can’t be viewed as having minor involvement in prescribing .The reality for me is that regulation is needed but not as set up presently. And who knows how that can be changed when there would be such well supported resistance from all the networks who gain by having them to fall back on. My problem with your argument is partly that doctors cannot be trusted to regulate themselves. Nor can companies. And when things do go wrong they have their own medical self interested defence groups and lawyers to support them . Most cases are not sexual abuse by individual doctors although that is not trivial and can be a sign of a culture of cover ups like the Jimmy Saville case The GMC and others were pretty negligible in that case. but they should and do now sometimes get it right by tackling what may seem minor cases to others.When clinical harms are covered up usually any complainant who even have the means to sue will be given the run around often for years. Individual doctors in the present tainted blood scandal whereby people have been injected knowingly with infected blood in a joint arrangement between UK and USA are not going to be sued, neither will any politician, regulator or company.
There are very few people who can like or admire Peter Doshi more than I do but that doesn’t mean I don’t think he has a terrible blind spot when it comes to regulation – he fails to understand it and he in particular made a disastrous hash of approaches to FDA in respect of the Covid vaccines that did none of us any favors.
The fact that doctors can’t be trusted to regulate themselves isn’t a reason to regulate them and certainly not by an agency whose job it is to monitor the wording of drug advertisements.
What is needed is legal action. Someone needs to work on how it might be possible to sue doctors in the UK and the rest of Europe and drug companies rather than have pathetic legal efforts like the effort to sue Astra-Zeneca for its Covid vaccine.
Chuang Tzu in 320 B.C. pointed to the error in the approach you and Tim and lots of others are advocating when it said – it makes sense to lock your property up with ropes and locks and bolts to protect it against robbers but when a strong thief comes along he picks the entire lot up and heads off with only one fear – that your ropes and locks and bolts will give way.
Your suggestions for more or tougher regulation will just make it easier for pharma to harm and kill with impunity. You won’t have to worry about doctors because they are doing themselves out of business.
D
Thanks Annie
The news headline is misleading in that MRHA is not going to probe links to suicide from Prozac and other antidepressants.
It is going to probe “the effectiveness of the warnings about suicide relating to antidepressants”.
“may contain nuts” will, I expect, be changed to “sometimes contains nuts” and the blame passed to the patients, their families/friends, and the prescriber’s malpractice defence organisation.
We need a different way of regulating in a way which is independent of the power of Governments and pharma and the medical bodies which collude with them. Not dominated by doctors themselves when their organisations are like moths or snakes whichever way we view them
– inclusive of other parts of health services and those who use them. The public has no power to protect themselves from these self protective set ups which lead to scandal after scandal. I don’t focus on it needing to be tougher or more regulation but certainly more humane. tougher or more regulation leads to bullying and positioning for power amongst networks as soon the organisation gets off the ground . The networks of medics who do speak out get sidelined or undermined or threatened or sacked It seems almost impossible to change things from within So we can can highlight how much they are a smokescreen all we want decade after decade . hopefully we might get a kinder more compassionate more honest medical and in general society based on values most of us share Pie in the sky maybe but it has to start somehow.
The Medicines and Healthcare products Regulatory Agency (MHRA) is an executive agency of the Department of Health and Social Care in the United Kingdom
MHRA funded by Pharma?
We do receive funding from the Bill and Melinda Gates Foundation as well as other sources outside government such as WHO. This funding mainly supports work to strengthen regulatory systems in other countries. The majority of our income comes from the pharmaceutical industry
How can anybody trust this kind of set up
When you say we need a different way of regulation or better regulation or tighter regulation or more regulations, it comes down to you are saying things are wrong and must change. There is no argument there – things are wrong and must change but it is pointless for you or me to keep saying things are wrong and we need change without specifying exactly what the problem is and what change is needed.
Kamran Abbasi, Richard Smith, Richard Horton and Peter Doshi say these things but they are dilettantes – they occasionally think they are brave and helpful to say things like this and brave to occasionally write angry pieces about an awful industry while being totally lilly-livered about actually publishing anything about adverse events for instance. Their lawyers won’t let them. When we get to this stage, we have a problem that ‘regulation’ won’t fix. We have a brute power problem. The pharmaceutical industry has all Western countries by the short and curlies.
The problem with dilettantes occasionally wailing about how awful things are – the dilettantes are all singletons with different ideas about what’s wrong, who only think about it occasionally and they are up against armies of lawyers working in company regulatory departments who strategize about how to use the next bout of pressure to put things right – to good effect – to make things even better for pharma.
Unless someone has a very good idea the best option is probably to do something that had all the good people like Bob Whitaker, Peter Doshi, Peter Goetzsche, Maryanne Demasi and others frothing at the bit at a recent proposal to have SSRIs made Over-The-Counter because they are so safe. Clearly they aren’t safe but they are much less safe because of all the regulations and guidelines put in place now to shape prescription only behaviour exactly to pharma’s liking. Unsafe though the chemicals are you would immediately cut through a lot of the regulations making them even more unsafe by making them OTC.
That’s what I mean by a concrete suggestion rather than just wailing or thinking in a dilettante fashion. The greater the push for more regulations, the bigger we will make Big Pharma and we will ultimately create Big Brother.
D
This matter is serious so I will have another go. Bid Brother and their sisters are already in post. I did make a suggestion above . Maybe it’s naive or useless but we cannot blindly accept that nothing is possible. Not sure f you were including me in the wailing and so on. Hope not I’m not in that class myself. We all make comments and suggestions on the posts which you write with hope they will be useful . But not necessarily always in agreement. Maybe those who get their views published have managed to bring about some changes whether dilettantes or activists but things are getting worse . Nobody has a solution which needs to be huge enough to overturn the networks in place now Chipping away is the only way it seems to be possible. But I definitely don’t want to go back to the days when doctors could get away with harming people without consequence using the ‘in my clinical judgement’ get out. Doctors not journals are best placed to speak out but they don’t .
Let me try one more angle. Regulation standardizes. This is its essence and it is the last thing we need more of at the moment – a standardization that claims the drugs work and are harmless and anyone therefore failing to prescribe them is falling beneath the standard of care.
A call for more standardization or more enforcement of standards can only make things worse. It will leave you and others like Louis Lasagna post 1962 figuring he had made a bad mistake pushing for new standards in drug regulation.
One way to give people more control is to make most meds OTC. Unless you can come up with something like this that will flummox pharma and undo a lot of what they have built up – anyone who just complains is playing into their hands.
Saying this is not to question anyone’s good intentions – least of all yours – but good intentions and virtue signalling are not enough. It’s far too late in the day for that
D
ARGUABLY, some of the greatest obstacles to patient safety, when it comes to antidepressants, are the intermediaries. Prescribers and regulators (companies) who intervene in the consumer-product DIRECT experience with overlays of medical authority, average patient response ‘data’, deliberate minimisation of harms like PSSD etc.
ARGUABLY, an OTC model for what has effectively become a ‘lifestyle’ drug, theoretical mood improvement for est 15% of the population, would be safer. How many consumers would persist in ingesting a product that claimed to improve their state of mind that rapidly made them feel dizzy, sexually and sensually depleted, numbed out and at worst agitated and even suicidal? Especially if the decision were entirely down to them, their personal responsibility for themselves or people they love – and not mediated by a medical authority figure and system?
ANSWER – probably, possibly, the minority for whom this class of drug seems to have real benefits. Know several people who have benefitted from ‘having the (emotional) edge’ taken off stressful circumstances (divorce, bereavement) over a short period, tapered and been fine. Estimates vary but we know up to 40% ditch the drugs within a few months because the adverse effects, especially sexual dysfunction, are intolerable.
There is a belief that the OTC /commercial world is unprotected and high risk. But, ime, having working in it for years across all kinds of product categories, the consumer is the judge and jury, crap products die fast – and regulatory is tough on claims. I cannot imagine the ‘chemical imbalance’ baloney would have stood a chance of getting through the net. And that was hugely dangerous and influential baloney, as we know – driving people to believe their unhappiness was in their heads and not in their lives and relationships, cementing continued usage and the belief they were ‘incurable’.
D.H. “There is no argument there – things are wrong and must change” –
I agree that looking to change Regulators alone would not achieve the progress required to prevent others suffering the deaths, injuries and disabilities resulting from casual, careless and ignorant prescribing of antidepressants/psychotropic drugs without valid consent.
When I asked: “Is it time to regulate the regulators” – I saw this as only one area where allegations of corruption and/or reports of links with the drug industry may result in prescribers being mislead, and may result in avoidable injury and death.
I had just watched Kim Witczac’s powerful (Consilium Scientific) You Tube seminar: –
‘The Spider Web of Influence: America’s Broken Drug Safety System’.
It was good to see Peter Gotzsche reinforcing the validity of prescription drugs (especially psychiatric drugs) as a major cause of death, and supporting Kim’s presentation.
I come from a family where four members of three generations died or had life changing injuries following: – misdiagnosis of malignancy, heavy metal poisoning from medical device failure, and SSRI induced akathisia misdiagnosed and mistreated.
Whist one was considered to be a regulatory failure (by a gifted barrister) I believe that to achieve change at the level we aspire to demands a campaign on multiple fronts. Changing the Regulators alone would clearly be incomplete.
Would the Normandy Landings 80 years ago have achieved anything if the invasion force had only landed on one beach?
Those of us who do what little we can to ‘attack’ on all the beaches have been inspired by those who founded RxISK, those who risked their careers and tolerated professional vilification for decades. (All The Good People). Their sacrifice and commitment deserves commendation.
I feel there is more agreement than disagreement in the above challenging debate.
The definitive comment to me is: –
“What is needed is legal action. Someone needs to work on how it might be possible to sue doctors in the UK and the rest of Europe and drug companies” – – –
Not perhaps impossible in most medical specialities, but with regard to litigation against psychiatry and psychiatric drug injuries, almost impossible.
When I realised the enormity of injury and destruction of life’s opportunities that psychiatric misdiagnosis and cavalier, enforced drugging had caused to our loved one, I approached an eminent legal practice in the UK country where it commenced.
The advice I received was:
“Let’s throw £5000 at it and see what happens”! This did not inspire confidence.
I have no doubt that (sadly) the most powerful lever for change towards safer medical practise is litigation.
It seems however that psychiatric malpractice is Medico-legally untouchable, and psychiatric drug induced death and maiming is exempt from compensating those patients and families that it has destroyed .
Psychiatry ‘Means Never Having To Say You Are Sorry’.
Tim
I figure most of us, including pharma and regulators have good intentions. But good intentions are not enough. I agree with pharma and regulators more than I agree with Peter Goetzsche.
Regulating the Regulators sounds nice but I think it might be meaningless. Regulators are bureaucrats – you want to add another layer of bureaucracy to what is already there?
When people like Peter Doshi call for regulating the regulators, I think they usually don’t understand what regulators do. FDA and MHRA and EMA are doing the job their job descriptions outline. When things go wrong its because you and Peter D and Peter G and BMJ don’t understand this and don’t understand how initiatives you likely once supported as the answer to problems with regulation – like installing randomized controlled trials – have backfired.
Other than legal actions and maybe better than legal actions, there are a few radical solutions – making drugs over the counter. This would create its own problems but would dismantle a lot of the current problem.
Another is bringing it to doctors and BMAs attention that doctors are going out of business. There is a growing clamour in BMJ about the replacement of doctors by physicians associates. This replacement was entirely predictable. You’re a doctor – you are in a much better position than most folk reading this blog to pull on this lever with a view to getting the kind of change that might make a difference. Have you ever thought about doing something in this area?
There are posts here and on RxISK blaming a succession of BMJ editors and BMA for creating a good deal of the current problems. Richard Smith knows he did a lot to put pharma in the commanding position they are now in but can’t bring himself to go public about it – perhaps you can think of ways to persuade him.
The Silencing Doctors, Silencing Safety post on RxISK points to a shocking scandal – that you and others could do something about. Specific somethings. Vacuous phrases like regulating regulators are going to get us nowhere
D
Thanks David,
I have just re-read Silencing Doctors, Silencing Safety. It would appear to be time to review my approach to advocacy. As a retired doctor, access to medical journals is limited but I may be able to address that difficulty via the RCGP Library.
This is the way it works – this is how FDA are covered and this is how Doctors are covered
The Bottom Line
‘A black box warning isn’t meant to completely rule out the use of a medication. Its purpose is to bring attention to important information. When you use it appropriately, a medication with a boxed warning can be a safe and reasonable treatment option.’
https://www.goodrx.com/drugs/safety/fda-black-box-warning
A ton of new warnings as the MHRA are going to be looking at will just give Doctors a ton of new protections.
It won’t deter doctors.
Increased risk of suicidality
The Food and Drug Administration (FDA) has directed manufacturers of all antidepressant drugs to revise the labeling for their products to include a boxed warning and expanded warning statements that alert health care providers to an increased risk of suicidality (suicidal thinking and behavior) in children and adolescents being treated with these agents1234. The boxed warning is for increased risks of suicidal thoughts and behaviors in children and adolescents with major depressive disorder and other psychiatric conditions who take antidepressants2. All antidepressant medications include a black box warning that details this risk5. Healthcare providers should monitor anyone taking antidepressants for changes in their behavior and mood5.
Despite FDA, above, these are just some of the deceased children
https://antidepeffects.wordpress.com/
Trying to hold doctors to account – They hold all the cards bequeathed to them…
‘ I would imagine that a great many such people and others on their behalf will feel extraordinarily let down and angry when faced with the evidence that I’ve been faced with.’
https://davidhealy.org/the-raine-in-june-falls-mainly-in/
If Yoko and Vincent can not find one doctor in France to support them, then burying the bodies, becomes hiding the bodies –
The Proof is in the Pudding…
No need to hold doctors to account – they hold fewer and fewer cards. They are going out of business. Even their medical journals like the BMJ don’t support doctors any more
D
Clinical trial for AI depression tool
https://www.bbc.co.uk/news/articles/c3geeljv84no
Prof Andrea Cipriani said he wanted to “treat individuals, not averages”
13 May 2024
Volunteers are required for a clinical trial where people with depression will be treated by an AI algorithm.
Oxford University’s department of psychiatry is testing the digital tool known as Petrushka, which it said would personalise antidepressant treatment.
It uses data from more than one million people and recommends, in real-time, the best antidepressants for each individual during a consultation.
The team wants to recruit about 200 participants by the summer.
The trial will involve more than 500 participants in total.
Petrushka uses information from each patient, such as age, gender and symptom severity, and takes into account side effects.
The researchers claim it is an “innovative way to empower patients and share decision-making during the treatment process”.
Chief investigator Prof Andrea Cipriani said: “In real- world practice, antidepressants are usually prescribed based on the clinician’s knowledge.
“There are more than 30 antidepressants on the market but nine times out of 10 GPs prescribe one of just four antidepressants.
“This means that patients may not get the treatment that would be most effective or sustainable for them.
“We want to treat individuals, not averages.
“We want to be as precise as possible and identify the best treatment for each patient sooner based on what we know works for patients with similar characteristics, rather than wasting time trying treatments that might be less effective.”
Patients can sign themselves up for the trial and a short screening process will follow.
It is also being carried out in Canada and Brazil.
Trial manager Nyla Haque said: “The study lasts 24 weeks in total but after eight weeks we will see how many participants are still taking the allocated treatment.
“This measure will tell us how acceptable and well tolerated a treatment is.
“We will also collect information from the participants about their mood, anxiety, quality of life and any side effects during the entire duration of the trial.”
The scheme is being funded by the National Institute for Health and Care Research.
Suicide ideation is high in adolescents.
Suicide attempts are high in every age if people is taking antidepressants.
Since 2015 more teenager girls (with psychiatric comorbidities) are going male (female to male transition) with more risk of suicide compared to the first wave of transexuals (male to female adults with 0 mental problems, with a lot of “tests” in the army in the War periods of XX’s century). Detransitioning multiply the risks in every sex. Being used as a guinea pig (John-Joan’s case) takes you to the same place.
Raping in youth cause a lot of problems always, in every moment of histort.
Having low OR “bad” social capital rise your feeling of isolation being surrounded by “strangers”. Social media only creates a “third field” [tercer entorno by Javier Echeverría] who push people to treat each other badly.
Being poor between poors has lower risk than being in the lowest socioeconomic quartile between richers.
If we center our analysis in the rise of technology, the dynamical stabilization of our lives causes pathologies of acceleration which, undermining our acceptence of the uncontrolability of the world, kills our ressonance (Hartmut Rosa).
Can anyone (more intelligent than me) fill the dots or add something new?
Conflicts of interest: I translated David Healy’s book in Spanish and I like how he explains things.
P.S: we need to add anorexia to the dynamical picture
https://segm.org/gender-dysphoria-anorexia-korte-gille-elective-affinities
Why don’t we allow girls to self-decide if they are fat or not (for girls with eating disorders they are never slim enough) but we permit to self-identify as being a male in the “wrong body”? We don’t make a liposuction as “slimness affirming therapy” but we can put them on puberty suppressing hormones, testosterone and double mastectomy / uterus extirpation being minors.
No reason given on the Government site as to why there is a time limit GOVUK I’ve read the situation in USA probably elsewhere too is different from the UK position They will be back possibly…Much anger about the decision from effected youngsters themselves being expressed through their own forums
In UK
New regulations restrict the prescribing and supply of puberty-suppressing hormones to children and young people under 18.
From:
Department of Health and Social Care
Published
29 May 2024
The government has today introduced regulations to restrict the prescribing and supply of puberty-suppressing hormones, known as ‘puberty blockers’, to children and young people under 18 in England, Wales and Scotland.
The emergency ban will last from 3 June to 3 September 2024. It will apply to prescriptions written by UK private prescribers and prescribers registered in the European Economic Area (EEA) or Switzerland.
During this period no new patients under 18 will be prescribed these medicines for the purposes of puberty suppression in those experiencing gender dysphoria or incongruence under the care of these prescribers.
The NHS stopped the routine prescription of puberty blocker treatments to under-18s following the Cass Review into gender identity services.
In addition, the government has also introduced indefinite restrictions to the prescribing of these medicines within NHS primary care in England, in line with NHS guidelines.
The new arrangements apply to gonadotropin-releasing hormone analogues – medicines that consist of, or contain, buserelin, gonadorelin, goserelin, leuprorelin acetate, nafarelin or triptorelin.
This action has been taken to address risks to patient safety.
Patients already established on these medicines by a UK prescriber for these purposes can continue to access them. They will also remain available for patients receiving the drugs for other uses, from a UK-registered prescriber.
Regulation
I had a concern over my mother’s treatment in hospital and after discharge- she was being coerced to accept a zolatronic acid infusion clearly stated in the clinical summery. I looked up zolatronic acid it didn’t look good and informed DH. Who replied ASAP. I reiterated the clinical summery to him. The reply from DH to me, in my view, probably stopped the coercion in its tracks. My mother has not been contacted by the hospital consultant at all since.
In my view just as in psychiatry many many patients in the same situation as my mother without the ability to push back have been harmed and pushed to an early death. It took just a short sentence from DH to stop it.