
This post ideally should be titled – Savoury or Saviour? – as will become clear. Its part of the Politics of Care forum. It follows What You Can do to Save the World in a sequence of posts about what a range of people from us to Politicians and Us can do to turn around the crisis posed by our growing inability to care for others when sick, when treatments go wrong, when they need social care or to care for our environment and climate.
One
Until recently doctors were there for us and our families first. They were much more than people who were a conduit to drugs. To get back to a position where we thought the Magic lay in them as we once did, rather than in the Medicines they now dish out in ever increasing amounts, they need to create Guidelines for People, the first element of which would recognize the need to contain medication burdens.
They need to get rid of Guidelines for Diseases primarily because these are harmful to us but also for the reasons laid out below – Guidelines for Diseases are largely based on a ghost-written literature with no access to the data from the studies claiming to support the treatments they prescribe – junk in other words.


Two
Doctors need to create or support deprescribing programs, aimed at reducing medication burden from more than five drugs, especially in older patients, to less than five. This will enhance the efficacy of the drugs the patient remains on and can reduce hospitalizations, improve quality of life, and extend life expectancy. See Introducing Taper MD and Five Minutes to Midnight.
There is a growing amount of deprescribing babble but less and less deprescribing in practice – partly because patient demand for more and more meds is growing – younger people in particular.
Deprescribing is not just a matter for older folk. Putting young people on antidepressants or other drugs they can’t get off will use up a medicine slot that may be needed in a later emergency. Explaining to a young person that drugs aren’t all they’re cracked up to be will be a challenge – you’ll find yourself called an old-timer who knows nothing about the latest research. Are you really up for the challenge?
Three
Life expectancy is stalled or falling and was before Covid. See Shipwreck of the Singular references for references on this.
If we are going to operate according to targets, why not target turning that around rather than the multiple targets for cholesterol, blood pressure, bone densities etc that we have at present that are making things worse rather than better.

Four
Insist on access to clinical trial data. There is none at present. No one gets to see the data – not the authors on papers reporting the results of studies, not regulators, not anyone. See Correspondence with NICE, the BMA, Brenda Hale, then Chair of the Supreme Court, Government Departments of Health – in From Stephen O’Neill to the Crack of Doom, The NICE before Christmas, The Death of Stephen O’Neill and The Perfect Killing Machine.
No-one gets to see the figures or the records. Data really means named people, not figures in a spreadsheet, or statistical outputs. If a death in a trial is coded death by burns, you will only know if the person poured petrol on himself trying to commit suicide and then died five days later from his burns if you have access to his full medical records or can interview his wife.
Without access to the data, we are not dealing with science – science is not about believing what some High Priest tells us. Any doctor who, in the current circumstances, tells patients to trust them because they are being scientific, may mean well but is essentially as fraudulent as the Wizard of Oz.
Five
Insist on full access to all healthy volunteer trials data with the ability to interview volunteers. These are the only drug trials. Clinical trials are condition trials where the effects of drugs and illnesses make it too easy for companies and regulators to duck a link between a drug and a hazard.
There are no confidentiality issues in healthy volunteer trials – other than commercial ones. Most of these trials remain completely unpublished and those that are published ordinarily omit adverse effects totally.
The suicidal and persistent sexual side effects of antidepressants were evident in healthy volunteer trials before these drugs were ever licensed and provided an early warning to companies on how to construct their clinical trials to hide problems like these.
Six
Support a change in the consent forms for clinical trials to mandate access to trial data. There is no ethical or legal basis to refuse this. The original clinical trial consent forms told participants they were taking an experimental drug – something they were not routinely told prior to that. Phrases telling people we will never show your data to anyone else, which sound good to trial participants, were inserted later by drug companies.
Seven
Encourage other doctors to ask companies for clinical trial data and to refuse to prescribe treatments that are not based on data. There is no science without access to the data. Companies need doctors more than doctors need them – if a group of you target certain drugs and refuse to prescribe without access to the data you can change everything.
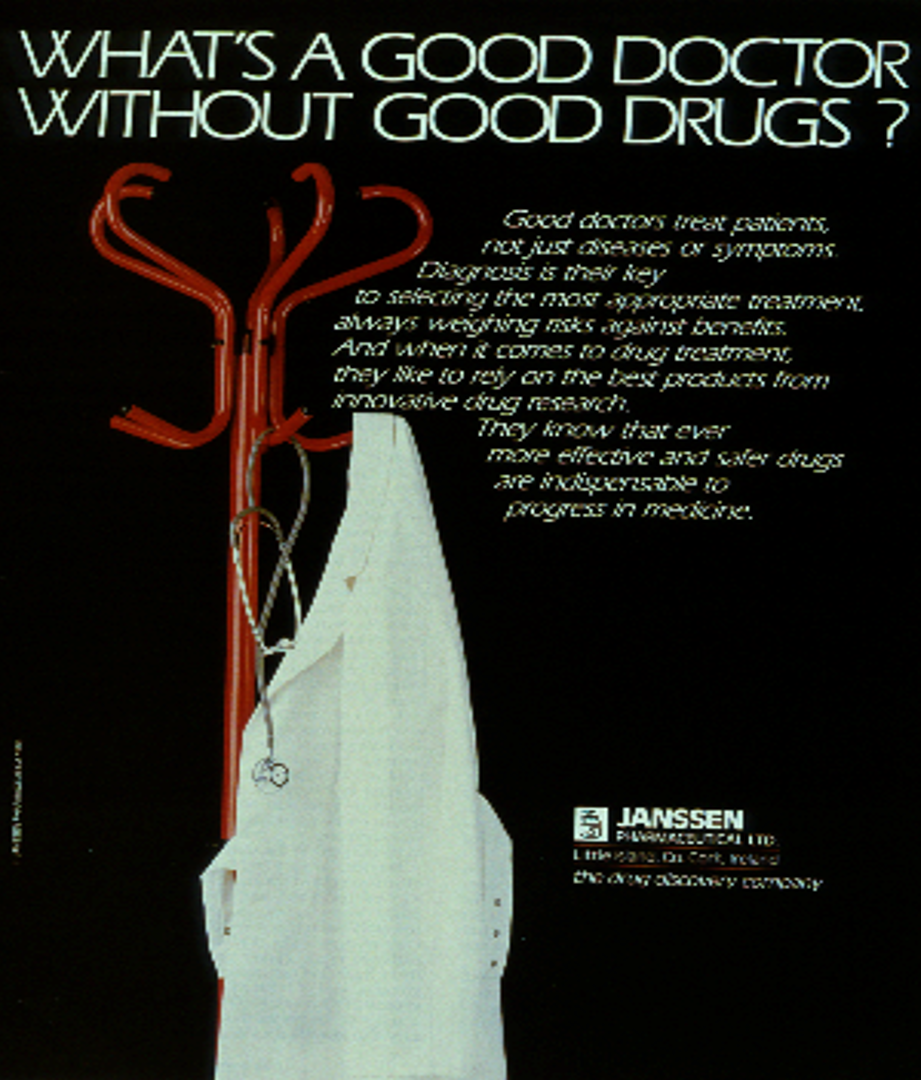
This was an advert for Risperdal before it was launched – the drug that helped doctors give pre-teen boys breasts and a company who played a big role in the opioid epidemic.
Eight
Ignore guidelines for drug treatments that are not based on access to data – they are advertisements. (Currently all guidelines are based on a ghost-written literature without access to the data. Guideline makers know this.) See The NICE before Christmas – and there is much more correspondence like the correspondence with NICE mentioned there where I offered them a phrase – its not NICE’s job to police the medical literature that they and regulators and health departments have leapt on ever since.
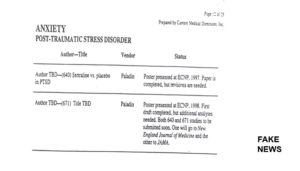
TBD means To Be Determined.
Nine
Require universities to tackle medical academics who put their names to medical articles without having access to and being able to share the full study data. This happens right across medicine but psychiatry as ever has led the way. A good symbol comes from Vienna, Freud’s old stomping ground, where the professor of psychiatry, Siegfried Kasper, is now a poster boy for just this kind of activity. The University of Vienna has refused to do anything about it. And the leading neuropsychopharmacology association, the CINP, recently made him their president.
In a similar move, the American Academy of Child and Adolescent Psychiatry made Karen Wagner their president, a woman who has testified under oath that most if not all of her articles reporting clinical trials have been ghost-written.
We are told we can trust people like these, and Charles Nemeroff below, because they have over 1000 articles to their name. See Tweeting while Medicine Burns, Tweeting While Psychiatry Burns and Burn Baby Burn.
If all of this is new to you and you know nothing about medical writing – you can get an astonishingly close to real life version of what its really like by reading Malcharist which is a thriller but like John Le Carre’s The Spy who Came in from the Cold is written with inside knowledge.
Ten
Learn about how to establish causality in the case of drug induced adverse events. This is not done by reading randomized controlled trial (RCT) results – RCTs are the gold standard way to hide adverse events. This is much more important than the passions doctors are trained to have these days.
Even God got around to realising Guidelines aren’t the way to go, when things go wrong. Mind you things didn’t work out so well when he did come down to take the training in person but you have no option. If you haven’t read it – read David Lewis’ Can we have some Courage in Leadership Please – from which the cartoon below comes.
Eleven
Report any adverse event a patient suffers on treatment leaving his/her name and your name on these events and indicating a willingness to be cross-examined. Leaving your name on these events will call for medical courage. It is not clear how many doctors have this kind of courage. But to adapt St Augustine, a doctor supported by a doctor has the strength of a Walled City.
Give a copy of any adverse event report you send to the regulator on an adverse event to the patient affected and encourage her/him to file a report also leaving their name on it.
Anonymous reports only help pharmaceutical companies – they do not help doctors or patients.
Being cross-examined is nothing to worry about. Regulators like FDA, EMA, MHRA remove patients’ names immediately and file your report away to grow mouldy. They are not about to get in touch with either you or your patient – the very last thing a regulator wants is any detail that might force them to connect a drug to a problem.
(Regulators are looking after the health of the pharmaceutical industry not patients. You are supposed to be putting your patient’s health ahead of company health).
Patient and doctor names on these reports transform them from hearsay into evidence. While regulators will do nothing, someone who is seriously injured by the treatment may be able to use a report with names on it in a way they cannot use the hundreds of thousands of other reports submitted to regulators, which get dismissed as hearsay.
Twelve
Report any adverse event on treatment to the pharmaceutical company that made the drug. If the patient was on a generic drug, report the event to both the original brand name company (who remain responsible for the drug label) and to the generic company.
Get your patient also to report to the relevant companies.
The report will ideally leave both your patent’s name and your name on it. Unlike regulators, pharmaceutical companies are under a legal obligation to establish cause and effect between their drug and any problem. They would prefer you to report to regulators and not to them – see A Call to H*ARMS, Extreme Reporting and Let’s do the AbbVie again. So do what they don’t want you to do.
The company should contact you and your patient. An approach from a company can be a fun and enlightening experience for both you and your patient.
See American Woman and American Woman 2.

Thirteen
If you ask your medical insurer whether telling a company that you think their drug has caused a problem is a good idea, they will likely advise you not to participate in this core element of medical care. Medical insurers would also likely advise you not to cross the road if you asked their advice on that.
If you make a mistake and consult your insurer and their response is a typical one, you/we will need to find a way to draw the attention of doctors more broadly to the fact that insurers are getting in the way of doctors being honest, advocating on behalf of our patients and saving medical business. We need to stop our insurers de facto supporting pharmaceutical companies rather than us.
Your courage will be called on at an inquest if one of your patients has died as a result of a drug you gave them. Your insurer will advise against telling the coroner that the drug caused the death. But this is the one place where you can make a difference. If you endorse a hazard of these drugs, it will make it easier for the coroner to make it difficult for the regulator and others to ignore it, which otherwise they will do.
See Do Not Forsake Me, Oh My Doctor.
Sodom and Gomorrah were destroyed because Lot – seen fleeing the city below – couldn’t find 10 just men. Saving medicine will require ten doctors willing to go against the advice of their lawyer and do the right thing by patients like Stephen O’Neill or Samuel Morgan. Lot’s wife ironically in this context is seen turned to salt- see below for the irony.

See If I find you ten just doctors… , Model Doctors? , Professional Suicide , Professional Suicide – The Clancy Case, Listen doctor and you shall hear, We Need To Talk About Doctors , Dance of the Sugar Plum Fairies: How prescription-only keeps doctors healthy and wealthy but not wise
Fourteen
Push for reform of the coronial system, so coroners record in an accessible archive the drugs people are on at the time of death. They don’t at present. When people die from Covid or vaccines for Covid, no one collects details of the drugs they were also on.
See Spotlight on the Suicides: the Coroner and From Stephen O’Neill to the Crack of Doom.
Enable coroners to indicate that a prescription drug may have contributed materially to a death. They can’t at present. Your testimony at an inquest can facilitate this.
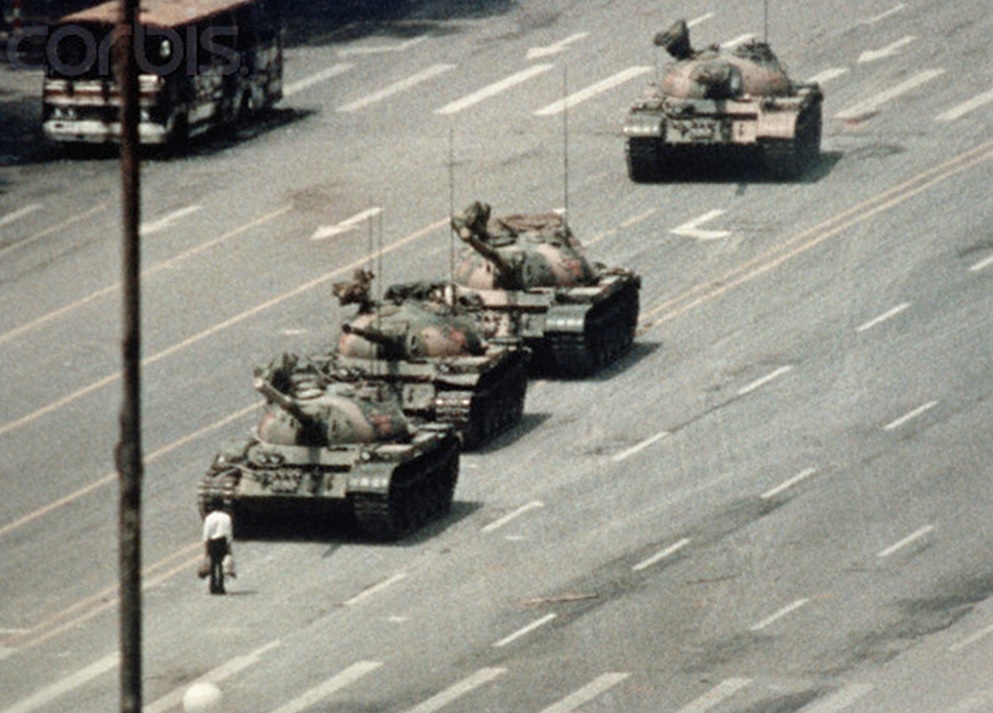
Coroners and you need to be able to follow a precedent just set by Pfizer. If anyone, in this case a young person, commits a gruesome suicide or homicide on sertraline – Zoloft, Pfizer will wheel out the Tiananmen Square tanks to blast the anti-science crowd away. But in clinical trials in 12-15 year olds of the BioNTech vaccine, some children became severely depressed on the vaccine, which Pfizer blamed on the SSRIs they were also on.
The medical – coronial system erases what actually happens patients when things go wrong as surely as details of what happened in and around Tiananmen Square in early June 1989 have been erased.
Fifteen
Consider submitting a RxISK Report on your adverse event and get your patient to file a complementary report.
Both you and your patient should consider notifying RxISK and giving us permission to let law firms acting for people suffering from the same or similar event that you have had contact you and/or your patient to discuss what happened.
There is a conflicting interest here. You and all other doctors are going to go out of business unless the powers that run healthcare can be persuaded that drugs are poisons and that it takes great skill to bring good out of the use of a poison, which warrants a better level of pay that just dishing out stuff per guidelines.
If medicines are sacraments that can only do good and cannot harm, then nurses of pharmacists are much cheaper prescribers and better because they are less likely to interrupt the managerial or political High Priesthood in the way a decent doctor might.
In the near future nurses and pharmacists and you will be replaced by prescribing robots. Robots may save more lives and reduce drug induced disability to a greater extent than you have been doing. If they do this, it will be because they take the feedback from patients more seriously than you have, and will reduced medication burdens.
So we are not asking for you to be moral – we are asking you or someone to be self-interested.

Doctors are on borrowed time. They make much too easy a living from the fact these drugs have been prescription only and we can only get them from doctors.
They ignore the fact that prescription-only is a police function and most of their patients get just as uncomfortable with them as doctors get with policemen.
The opioid epidemic has shown that medical common sense or values no longer exist. Too many doctors now dish out too much stuff that many patients can see is not sensible. If patients could get their meds over the counter, how much business would doctors still have? If the answer is not much, doctors need to think about what it might take to make them attractive to people who could get their drugs elsewhere.
Sixteen
If you agree that drugs can cause adverse events, we have begun a set of RxISK Maps that locate doctors willing to agree that drugs can cause problems and willing to work with people to establish what is happening on treatment.
If this can be developed it may be good for medical business. If the ‘market’ works as it is supposed to do, a Map showing patients where to go to get savoury medical input, should slowly bring other doctors around to recognising the need for them to agree drugs are complex things that can cause problems. Enabling them to remain in business too and support you in the process.
See RxISK Map: Professionals who just want to have Fun.

Seventeen
There is a good deal of emphasis these days on Choosing Wisely. A lot of doctors sign on to the need to avoid unnecessary tests and procedures, although the services in which they work may not.
A wise choice is probably more likely if there isn’t a measuring instrument of any sort in sight. See The Macbeth Test. If you have taken to rating scales or checklists or admit into the conversation a checklist a patient uses, the option to choose wisely will rapidly close. Companies know that figures for which their drugs can be pitched as an answer are the best way to drive sales – its the first step in their act of hypnotising us.
Its being able to sit in a room with another person and really listen without turning to a technique that might save doctors jobs. It might also provide a template for saving the world. Saving the world is about getting back to embedding techniques in judgement calls we make rather than having techniques de facto make the judgement calls for us.
Eighteen
The image here is a symbol of the Cochrane Collaboration and is touting RCTs as the gold standard in evidence, something that offers doctors a shield to battle against every possible bias that might compromise their judgement.
Cochrane don’t let you know that they build their reviews of drugs on a ghostwritten literature and that when they had a chance to push for access to trial data, they flunked the challenge.
But even if Cochrane had a spine and trials were done by angels, there would still be a problem. RCTs evaluate a primary endpoint – one of the 100 effects every drug has. They are therefore by definition not a good way to evaluate a drug.
They are the gold standard way to make adverse effects vanish. The people who most commonly exhort doctors to practice evidence based medicine are pharmaceutical companies.
For more on the limits of trials, see
- Sex and Evidence Based Medicine
- Does my Bias Look Big in This
- The Fault Lies in Our Stars
- Fawlty Stars
- Clinical Trial Fraud
In just the way we fetish guns and drugs figuring they kill or heal, when we do the killing and the healing, doctors and the system now fetish RCTs. RCTs supposedly make the right judgement calls. If we don’t make the judgement calls, they aren’t going to be right.
We is a key word here. Fetishes didn’t have much to do with sex before Venus in Furs, written 150 years ago. In this Leopold von Sacher-Masoch concludes that until women were as powerful, educated and wealthy as men, the relations between men and women wouldn’t be right – men would default into fetishes among other things.
Between access to the Internet and having skin in the game when things go wrong on treatment, many patients taking problems to doctors are better educated than they are.
Doctors increasingly have a choice between a job that involves 100 heartsink patients and twisted relationships, or having fun collaborating with 100 free researchers. If you are really relating to the person in the room with, you will find yourself able to put to one side any fetish with RCTs you may have been leaning toward.
Nineteen
The greatest scandal in medicine today is that there have been 30 RCTs done in children who are depressed – all of them negative, including those published as roaringly positive, yet doctors are dishing these drugs out like smarties. The ghost-written academic literature has led to the greatest known divide in medicine between what the Bible says and what the facts on the ground say if they are accessed.
Despite this, antidepressants are now the second most commonly used drugs by teenage girls – many of whom won’t be able to get off them, who will be unable to make love while on them, who will miscarry if they do get pregnant and if they don’t are more likely to have a child born with physical or mental handicaps.
The full story of how this happened is told in Children of the Cure.
Doctors need to work out a way to get back to the kind of street wisdom Homer Simpson shows below. This isn’t easy. Don’t let talk of Shared Decision Making fool you, or think because you read articles about adherence rather than compliance that things will be okay. If you try this out, you will find yourself swimming against an increasingly strong cultural tide – particularly among young people.
You can go with the flow or you can you look after patients. If you opt to look after patients, there is little option but to Man UP.
Finally
If salt loses its savour what good is it to anyone? We don’t need our doctors to be saviours but we do need them to be savoury.

Posts to come will cover what Politicians can do, what the media and others can do.
These ideally need to be drawn to the attention of politicians who whatever their background are the only ones that can get the kind of debate that is needed going. Of course one way to draw it to the attention of politicians is for a doctor to refuse to prescribe without access to the data.
Unite the union They want to save the NHS – but how many are even alert to `the harms described in the posts which are being caused whether in USA or UK. I read that this phrase was written initially in the bible but an Irish clergyman-political activist said it as a wake up call in 1705. “Eternal Vigilance is the Price of Liberty” Kind of a depressing but true comment on humans societies; ability to live together
NHS for sale
Takeover of London GP practices by private US healthcare company could face judicial review, says Unite
Thursday 1 July 2021 Share.
Campaigners, including members of Doctors in Unite (DiU), have ‘crowdfunded’ about £40,000 towards a possible judicial review regarding the recent takeover by Centene’s UK subsidiary Operose of the privately-owned AT Medics set up in 2004 by six NHS GPs and which runs 37 GP practices across London.
The campaigners are waiting to hear if all the legal hurdles have been crossed and the case can proceed on the basis of the lack of transparency.
Doctors in Unite chair Jackie Applebee said: “Ministers and senior NHS executives have repeatedly mouthed the mantra that the NHS is not being privatised, but that is patently not true as the awarding of lucrative contracts to private healthcare firms continues apace.
“We are now hoping to test this policy with a judicial review as to why a huge swathe of English general practice, including the data of nearly half a million patients, was handed over to US health insurance giant Centene – with a breath-taking lack of transparency and openness. We have been told by the lawyers that we have a strong case.
“The new health and social care secretary Sajid Javid needs to be made aware of the strong groundswell of public opinion against the accelerating pace of NHS privatisation presided over by his disgraced predecessor Matt Hancock and he should immediately reverse the hiving off of NHS services to profit-hungry healthcare companies, such as Centene.
“The public needs to wake-up to the fact the NHS, whose 73rd anniversary we celebrate on Monday (5 July), is being steadily sold off to profit-hungry healthcare companies – in this case one whose headquarters is in America.
these founding principles of the NHS in 1948 will become mere ghosts of themselves.”
Xcellnt UNcommon sense.
Cure for Leukaemia? Metformin and one blood pressure med….. Will the lady even listen to me? No. Trusts the experts….
An Aussie doctor recently injected 50 grams not mg, grams, saving patient from sepsis.
Have a great life!
From previous DH post – ‘Care’ Homes: What is Care?
July, 4,
‘Another more recent response from management and politicians has been to focus on vaccinating care home staff as the answer. This technical solution to a people problem in between the lines blames people whose behaviour has been dictated by poor pay. A solution more appropriate for bodies than for people.’
In France Care workers have already been told they must get vaccinated.
In UK …
🚨 URGENT MANDATED VACCINES – CALL TO ACTION 🚨
Inbox
Save Our Rights UK sorukadmin@saveourrights.uk via mlsend.com
12:17 PM (7 hours ago)
to me
Today the Government have snuck a Statutory Instrument onto the program of the day that would mandate vaccines for all care home workers. This would include not only the staff looking after the residents but also all cooks, cleaners, handy men and so on. This would result in thousands of people being forced to have the vaccine and hand over their private medical information to their employers.
Over one third of care home workers have said that they will consider quitting their jobs if the vote passes today. Lets help them feel safe to keep their job by urging MP’s to stand up for medical freedom and to vote against this motion.
It takes less than a minute and a half to send an email to your MP here.
If you have more time after that then please also consider retweeting our Call to Action on Twitter and sharing the Facebook post too.
Many thanks for standing with us for Medical Freedom.
Kind regards,
SORUK Team
2 of 5
Mandatory Covid vaccinations (Case Ref: BW3495)
Response from MP
Beth Winter MP
1:22 PM (6 hours ago)
to me
Thank you for getting back to me.
I will be voting against the Draft Health and Social Care Act 2008 (Regulated Activities) (Amendment) (Coronavirus) Regulations 2021.
I am against the principle of mandating any sector of society to receive the Covid-19 vaccine and also in practice I am aware that any mandating of the social care sector to take the vaccine to enable staff to work will lead to significant staff shortages.
The Labour Party shares this perspective and as has happened in Wales prefers to encourage people to take the vaccine rather than making it obligatory.
Yours
Beth
Beth Winter MP
Seventeen
Choosing Wisely
Head First – by Alastair Santhouse review
In a passionate blend of anecdote and evidence, a consultant psychiatrist shows how the mind and the body are irrevocably connected, despite medicine’s desire to separate and specialise
https://www.theguardian.com/books/2021/jul/14/head-first-by-alastair-santhouse-review-a-medical-memoir-with-elegance-and-integrity
“Nothing is more fatal to health than an over care of it,” Franklin said, and Santhouse uses this wry 18th-century observation to set a series of interesting challenges for his readers:
“Medicine fulfils the function of legitimizing illness because, as a society, this is the role we have chosen for it.” Santhouse writes, hypothesising that this is why, in the last 60 years, the American Diagnostic and Statistical Manual (DSM-1), which lists all known mental illnesses, has leapt from a modest 128 categories to a very generous 541. We are clearly on a desperate crusade to be labelled. But the problem with labels, Santhouse states, is they can often be sticky and impossible to remove.
Simon Wessely Retweeted
Alastair Santhouse
@Dr_psychiatry
It’s always a nervy moment reading your first book review – and it’s hard to put into words how happy reading it made me
‘He does not shy away from difficult themes. He addresses suicide, end of life care, chronic fatigue
‘Head’ First – always a nervy moment …
One more step for for women. Oral contraception can now be bought at che .mists, People would probably be safer getting more drugs from them and likely underage girls wouldn’t get access to harful contraception so easily. Without the ‘authority ‘of heartsink medics and their never ending prescriptions maybe more would throw them down the toilet sooner when adverse effects began to show- maybe more attention would be paid to info about them ,before getting serious addicted. They are too useful cashwise though for them too give up repeat consultations and get ‘them’ out of the room.
I don’t think There are any UK doctors on the Rxisk Map – from the survey being conducted by Pulse Today it seems they don’t consider the nitty gritty of medicine ,such as looking into the data would be ,as part of their job – they insist on being ‘generalists’ not ‘specialists’ an attitude which lets them off the hook.
How about some UK doctors who support Rxisk maybe behind the scenes, contributing something more than the woolly self interested stuff that has been gathered so far. Clare Gerada is on the panel so spokes in the wheel are likely but it might ring a few bells with some of the others panelists? We as a society need doctotrs on our side – too often they are not especially those at the top of hierarchies.
Building Better campaign: What services should general practice offer?
Building a Better General Practice
09 July 2021
We have completed the first part of our ‘Building a Better General Practice’ campaign, looking at the role of the GP. Today, we launch our second survey, where we ask readers to determine what services GPs should be offering, having already met with our panel of experts and grassroots GPs.
Take the second survey here
Conclusions from first survey on the role of the GP
ScienceMag.org
Contents
Current Issue
European law could improve ‘scandalous’ lack of clinical trial data reporting
By Barbara CasassusJul. 14, 2021 , 11:25 AM
The global pandemic has turned a spotlight on clinical trials, which test thousands of drugs and therapies each year. In Europe, however, the enthusiasm for trials is not matched with a zeal for reporting the results to the public. A total of 3846 European trials—nearly 28% of 13,874 completed trials in the EU Clinical Trials Register (EUCTR) on 1 July—had not posted their results on the register, according to the latest data from the EU Trials Tracker, set up by U.K. researchers in 2018 to expose lax reporting. Public research hospitals and universities, not drugmakers, are responsible for the vast majority of the lapses, which appear to violate European rules that require sponsors to post their results within 1 year of a trial’s conclusion.
“It is scandalous not to disclose the data, however disappointing, to the patient participants, to taxpayers in the case of public funding, and to everyone else involved,” says Florian Naudet, a metaresearcher at the University of Rennes hospital in France. Naudet says undisclosed results can lead to wasted efforts and missed signs of drugs’ potential harms.
But Europe is getting more serious about enforcing the reporting requirements. The European Medicines Agency (EMA) has stepped up reminders to trial leaders, and a new trial registry is set to come online in January 2022, when national regulators will also gain more power to enforce the rules. The shifts dovetail with signs of change in the United States, where many trial sponsors are also remiss: In April, the U.S. Food and Drug Administration (FDA) for the first time cited a violation of a widely flouted U.S. public reporting law.
Till Bruckner, founder of TranspariMED, a U.K.-based advocacy campaign to improve reporting, is hopeful that, soon, he won’t have to chide trial leaders so much. “I’m sick and tired of doing regulators’ jobs.”
from Aljazeera
Opioid maker J&J, distributors near $26B deal with US states
Along with Johnson & Johnson, the proposed settlement includes distributors McKesson Corp, Cardinal Health Inc and AmerisourceBergen Corp.
McKesson, Cardinal Health and AmerisourceBergen already indicated in regulatory filings that they expect to pay $21bn, and Johnson & Johnson would pay $5bn [File: Mark Lennihan/AP Photo]
McKesson, Cardinal Health and AmerisourceBergen already indicated in regulatory filings that they expect to pay $21bn, and Johnson & Johnson would pay $5bn [File: Mark Lennihan/AP Photo]
By Jef FeeleyBloomberg
20 Jul 2021
Opioid maker Johnson & Johnson and three drug distributors are expected to disclose this week the final terms of a $26 billion settlement for thousands of lawsuits accusing them of fueling a public-health crisis, according to people familiar with the deal.
After years of negotiations with five states, the companies are poised to make the announcement Wednesday, according to the people who asked not to be identified discussing closed-door talks.
We are a team of nearly 48,000 mission-driven partners striving each day to advance healthcare and improve lives. We are Essential to careTM.
Headquartered in Dublin, Ohio, Cardinal Health, Inc. (NYSE: CAH) is a distributor of pharmaceuticals, a global manufacturer and distributor of medical and laboratory products, and a provider of performance and data solutions for healthcare facilities
AmerisourseBergen (- also loves animals- so sweet)
We are united in our responsibility
to create healthier futures.
As we pursue our purpose, we make a positive impact on the health of people and animals around the world.