
This post was delivered as a Medicine in Crisis lecture at a Pills and Skills for Depression meeting that David Antonuccio organized in Reno Nevada on October 4. Kim Witczak who features throughout the post was a panellist at the meeting. There was an audience of over 200 primarily University of Nevada students – so the talk is not like a tight academic article, it is emotional and hoped to enlist their input and the input of their generation to solving our problems.
There will hopefully be a video recording of the entire meeting with David A’s talk and the panel meeting with Kim that cut to the chase, which will ba availabile. Meanwhile I made a video recording of my input soon afterwards which can be viewed here:
Health, Science and Care
I was in Houston for the Bicentenary – 49 years ago. A few of us were working to pay our way through College. Houston had just opened up what they claimed was the highest steepest Big Dipper ever. I’d never been on a Dipper.
One of the gang suggested a bicentary ride. I was paired with Greg, who had been on one, and was the coolest dude I knew, so it was odd to have him say you will be petrified at the Top. I was and still haven’t recovered a memory of the drop.
This talk is a Dipper but I’m not trying to give you a Near Death Experience. You may get a jolt or two but nothing compared to the jolt Kim Witczak got when her husband Woody with no hint of prior nervous problems, had a few nights poor sleep, for which he was put on a Big Zoloft Dipper. Woody died on the Dipper.
Here are things you’re told you’ll learn from us. Learning from us is very last millennium.
We are 9 months to the day to the 250th anniversary of the Declaration of Independence, hopefully enough time for one of you to conceive of and give birth to actions that might keep us all alive when we ride a Healthcare Dipper – might free us from the Unsafe Safety System we now have.
Four Dips
In the 1980s, an NIMH trial compared the first antidepressant imipramine – this was pre-SSRIs – with Cognitive Behavior Therapy (CBT), Interpersonal Therapy (IPT). The control group combined a placebo relationship and placebo pill.
CBT and IPT did not beat relationships. Imipramine was better but only in severe cases. SSRIs are weaker than imipramine and useless in severe cases so would have lost out in this trial. CBT folk seemed less likely to relapse than imipramine folk, and relapses would be even more true with SSRIs which have nasty withdrawal problems. But if CBT and IPT didn’t beat placebo, what did that mean?
It looks like on average we do best if we get better under our own steam or Care for each other.
In the case of medicines with side effects, if you don’t beat placebo you’re doing worse. Even with a short term gain you may be worse off. But is this true for therapy where you learn skills?
Dip 2
SSRIs claim to correct lowered serotonin or chemical imbalances and fix your broken brain. In fact, they will make your prior normal serotonin system abnormal, perhaps permanently.
CBT claims it corrects your dysfunctional attitudes and misattributions, your broken mind. But the NIMH study showed people with fewer dysfunctional attitudes or misattributions did better with CBT than those with lots. And the NIMHers who did best on IPT had the least interpersonal problems to begin with.
You risk having a normal you made abnormal by having what 9 times out of 10 are political problems – Us problems – located in you. Whether Pills or Skills, Therapist or Doctor:
Beware, beware.
His flashing eyes, his floating hair!
Weave a circle round him thrice,
And close your eyes with holy dread:
For he on honey-dew hath fed,
And drank the milk of Paradise.
David Antonuccio’s talk illustrated and this talk will identify The Milk of Paradise that puts you at risk.
Dip 3
Surely CBT doesn’t cause harms – suicides, homicides and permanent sexual dysfunction – on an SSRI scale? Well when you don’t respond to CBT or IPT, therapists rarely say maybe we should never have started. They add ACT, DBT, etc and refer you for meds – off which you might never get.
During the 1980s and 1990s, CBT and IPT therapists wrecked tens of thousands of families and lives by recovering memories of abuse that never happened. Therapists believed stories of abuse on alien spaceships at the age of 1 – buying into this threatens the sanity of your patient and colleagues.
Recovered memory hasn’t gone away. We’ve now got trauma informed care and complex PTSD. These are the psychobabble equivalents of the low serotonin and chemical imbalance biobabble.
David elegantly divorced the skills and pills from the people we get them through. .
But if Woody had taken a potent SSRI like chlorpheniramine that can cause suicides, sexual and withdrawal problems, he would be alive now. How come? Well if it didn’t suit him, he got it over-the-counter and would stop. His doctor insisted Woody continue taking Zoloft. Doctors may even double the dose or detain you if you mention crazy thoughts in your head.
Houston – we have a practice problem.
Dip 4
Study 329 was published on the 225th anniversary of the Declaration of Independence. This study of Paxil in depressed teenagers is the best Symbol there is of our Unfreedom. This was the archetypal instance of a negative trial being published as positive. Despite a fraud charge and $3 Billion fine, it remains unretracted with downloads costing $41 and its owners, Elsevier, making $3.5 Billion per year. It’s still built into Standards of Care. See Children of the Cure.
The literature on all our medicines, not just SSRIs, is ghost-written.
I was the grant-holder for a 1990s RCT of CBT for delusions. We had two CBT luminaries on the grant. Our article claimed CBT worked. In the virtual world of Rating Scales, there was a change you could call a benefit. But in the real world there was no sustained benefit. I suggested a follow-up article. The gurus panned it. CBT for psychosis doesn’t work.
When they don’t work for severe cases of a problem, lots of psychotherapy articles get left unwritten, along with articles on TMS and other Neuromodulatory treatments for nervous problems.
This fits with something else. Common diseases like Rheumatic Heart Disease can disappear – probably linked to antibiotic overuse. Catatonia disappeared probably linked to overuse of benzodiazepines. Classic Post Partum Psychosis has vanished. Schizophrenia is also slipping away. But no one wants to know why.
We once made Weapons to fight Wars. A realisation that We now make Wars to sell Weapons began to dawn with World War 1. We once made Treatments to fight Diseases. A realisation that We now make Diseases to sell Treatments began to dawn with the SSRIs.
SSRIs transformed a rare disorder for which we had good treatments into the greatest source of disability on earth, which like Hotel California you can check out from any time you like but never leave.
No one is interested to see diseases disappear.
A Bump
Four years ago, Joanna Moncrieff and Mark Horowitz, psychiatrists psychologists see as almost honorary psychologists, wrote an article for Social Science and Medicine, noting that 29 of the 30 most cited antidepressant publications referred to an established serotonin abnormality in depression but offered no evidence for one.
Asked to review it, I confirmed there never was a serotonin abnormality and suggested the editor could kill two birds with one stone. The reason 29/30 make a serotonin claim is they are ghostwritten with ghostwriters citing each other and a marketing message they’ve been adding to articles for years. Get the authors to mention this.
The editor loved the idea but the authors were too nervous to state the obvious, so she asked me for a short piece to publish alongside their article.
I wrote everything she wanted but I knew the Bump would discombobulate her too much to publish. I added that what applies to SSRIs applies also to the Covid vaccine trials in the New England Journal of Medicine, which are ghostwritten, with no access to trial data and evidence of injured patients disappearing.
I have had friends killed and injured by these vaccines. Friends, who were such true believers they participated in these trials, were injured and disappeared. I was working in a clinic where staff had to get vaccines and some were clearly injured but told by colleagues they had to get second doses because their problems were not vaccine related. This was a repeat of Woody’s problem.
In the case of Therapies, when told to, as we did in Germany 80 years ago, we get on trains heading East. If we figure things don’t seem right we also figure someone will realize a mistake has been made. This doesn’t happen. When survivors got to Israel after the War they were not met with sympathy – why didn’t you resist they were asked?
I have never suggested anyone not get a vaccine or asked for any drugs to be removed from the market. Vaccines and SSRIs are the same story. (Where does the Misinformation come from). My concern is that confidence in treatments is important and we risk losing it. To be appropriately confident we need to be allowed to be wary.
There is something we need to resist but what exactly?
Ascending
We have come to the Steep Slow Ascent and have time to ask – Where did SSRIs come from?

Medical Freudians 60 years ago seeing patients on antidepressants like imipramine could spot them becoming suicidal or homicidal, which cleared on stopping and reappeared on restarting treatment. Doctors can’t spot this now.
The analysts could separate the sexual effects of meds from severe mood effects. Doctors now can’t spot the sexual effects of drugs that completely wipe out the ability to make love ever again in mildly depressed folk who had no sexual problem before starting the meds.
On some of these antidepressants, the analysts could spot a change in what they called transference reactions – a change we now call reduced emotional reactivity.
Arvid Carlsson, a Nobel Prize winner, noted they reported this on antidepressants inhibiting serotonin reuptake but not others. So he made an SSRI.
For Carlsson, just like LSD, SSRIs acted on a normal serotonin system and can give some a good trip and some a bad trip. Reducing affective reactivity by the right amount is good. Can SSRIs make people suicidal? Yes – Carlsson said.
Carlsson did not see SSRIs as Magic Bullets that restore the correct factory fittings. SSRIs were Therapeutic Principles.
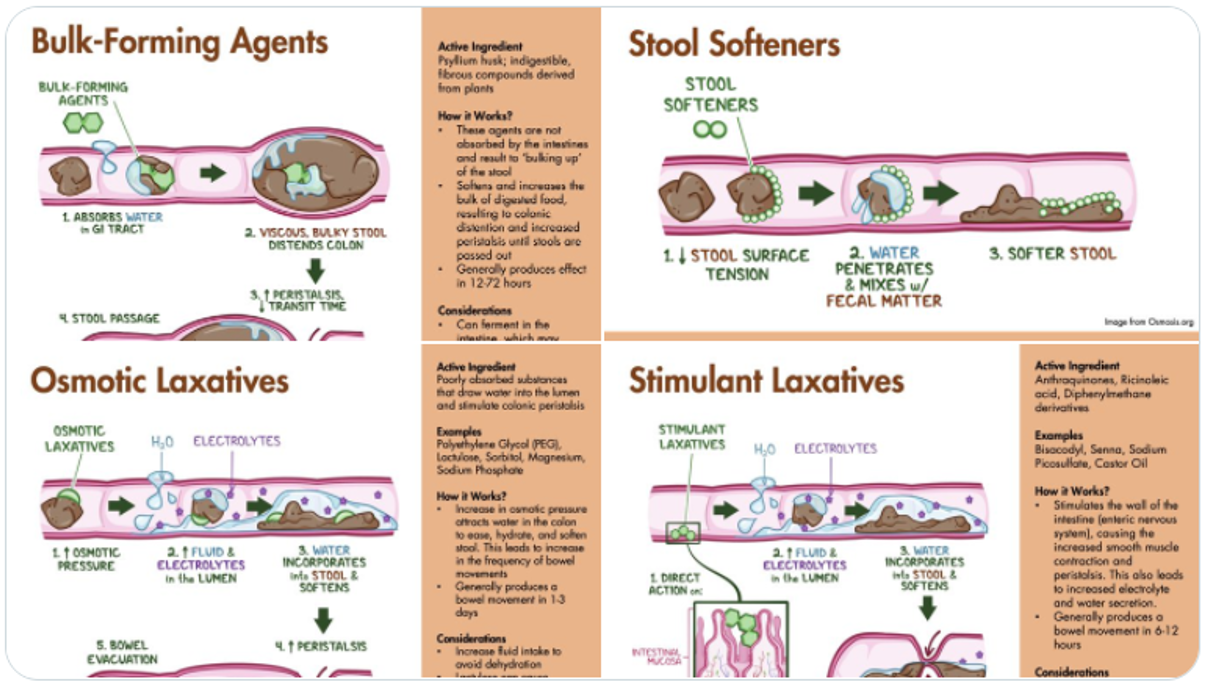
There are 4 kinds of constipation and 4 laxative principles. You can add fluid or bulk, stimulate or relax the gut. There’s a right principle for your constipation. The wrong one can make things worse. Great grandmothers and old-style family doctors could get this right.
But a company licensed to use the word laxative doesn’t mind if you’re on 4 laxatives provided one is theirs. This way treatment resistant constipation lies. Ditto for any medical problem including depression with euthanasia increasingly the only way out of SSRI induced treatment resistant depression.
You expect Drugs used as Therapeutic Principles to be put in your mouth and act on a spot in the brain. But benzodiazepines, beta-blockers and nicotine work by fooling our brains. Benzos relax muscles and fool brains into thinking we aren’t anxious. Beta-blockers slow heart rates and fool us. But beta-blockers can increase heart rates for some creating anxiety. At this point we need someone who is working with us rather than from a book.
Did I say nicotine?
The reduced emotional reactivity SSRIs cause is more useful for OCD than depression. Arvid Carlsson didn’t treat patients but he listened when told by a clinical colleague some folk with OCD claimed nicotine was more helpful for them than SSRIs. He helped run a trial which showed some of us do better on nicotine.
I’m not advocating nicotine – my father died prematurely from lung cancer. Fathers of friends did too or from heart attacks. But SSRIs also kill prematurely.
If you have OCD, who’s best placed to decide what is best for you? FDA? Me? Only you can compare any benefit you get with nicotine and SSRIs and weigh this against the risks.
We all used to be able to say the Art of Medicine aims at bringing good out of the use of a poison, but now liberal elite audiences in particular hold a crucifix and garlic up in front of me and hiss if I say this. Nicotine maybe brings home a point. It also suggests a fundamental change in how we view medical inputs since I began.
Therapeutic principles apply in psychotherapy also.
Freud’s initial principle was to believe patients who mentioned sexual abuse but when a woman threw her arms around him, he came up a new principle – transference reactions – her fantasies about her father. This elegant new principle got in the way of him recognizing sexual abuse. Freud’s 2.0 principles aren’t much good for us but are great for companies who use our need for a father figure to get us and our doctors to defer to bureaucrats in FDA rather than see someone like Woody being ab-used by meds. If Woody mentions weird thoughts in his head – that has to be fantasy.
Jung didn’t agree that Freud’s logic applied to all of us. Extraverts when anxious share their problems around, he said. Introverts retreat into their own heads. This sounds ‘mental’ but your degree of extraversion-introversion predicts how much anesthetic it will take to put you to sleep for surgery – extraverts need much less.
Extraverts, like Woody, are less likely to respond to SSRIs, while introverts are more likely to get OCD and respond.
Extraverts now get labelled as ADHD and introverts as ASD. Pathologizing normal variation like this is a disaster.
Figuring we all should be logical, Beck’s CBT has been poor at recognizing the greater susceptibility of extraverts to memories of abuse that never happened.
Like many drugs, CBT combines several therapeutic principles – cognitive restructuring, problem solving and behavioral activation – only one of which might be right for you but it all gets forced on you by therapists who stick to the manual.
The Art pf Psychotherapy is bringing good out of Brainwashing.
The pharmaceutical industry have been the masters of Therapeutic Principles – they call them Marketing Principles or Segmentation. Industry know consumers aren’t all the same – extraverted and introverted consumers need different approaches. They describe 4 different kinds of consumers. But for industry you guys listening or reading are not the consumers – prescribers are the consumers.
You might put drugs in your mouth but we make the money for industry when we prescribe. Never in the course of human history has there been such an amount of marketing dollars spent on such a small group of consumers as is spent on doctors – not money into our hands, money aimed at creating what gets called evidence.
Back to SSRIs – do these also fool our brains?
Less than 5% of our serotonin is in our brains – the bird-brain bit. 95% is in our sensory nervous system – our eyes, ears, skin, joints, muscles, blood, gut and genitals. Our sensory system – not our brains – is the boundary between us and the world. This is where Daniel Kahneman’s Fast Thinking takes place. Our Slow Executive Thinking might catch up later and can be badly mistaken – like Freud’s analytic ideas.
LSD and SSRIs work on the serotonin in our sensory receptors. LSD famously opens the doors to sensation – flooding us with sensations from our guts, skin, joints, eyes, ears and nose, loosening our associations by disturbing a gate-control. Too much sensory input can seem to put us in God’s presence and leave many believing in an afterlife or inter-generational trauma.
SSRIs close these doors. 30 mins after a first pill, SSRIs numb your genitals. Your senses generally, vision, hearing, balance and pain are also muted; you don’t react as much and get fooled into not worrying.
Rather than loose associations and intuitions, tuning down sensory input can give us tunnel vision that leaves us more open to suggestions from therapists about intergenerational trauma – more open to hypnosis. It’s like a sensory deprivation tank.
This is about to become a more serious problem as LSD and mushrooms get licensed in therapy packages – aimed at making money rather than keeping people safe
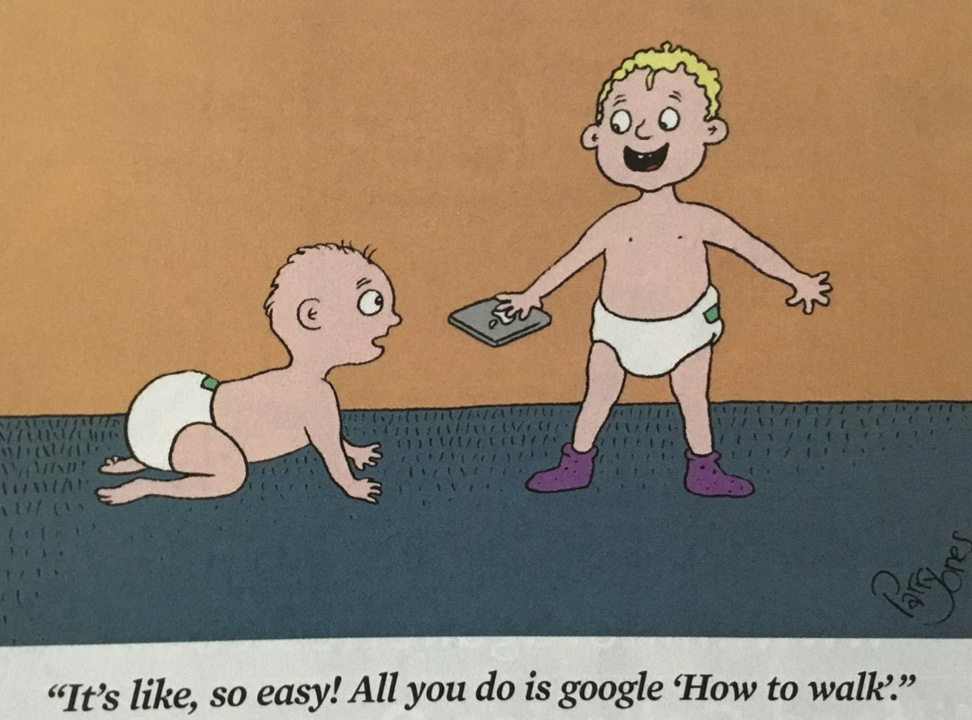
When SSRIs damage us, we experience Brain Fog and think our brains are broken, but tests show our brains working normally. Our performance is broken – the knowledge in our vestibules, joints and genitals is broken. Cognitive efforts to fix the problem by close attention and concentration are effortful and we call this Brain Fog. Embodied learning is what gets 1-year olds walking. They can lose the skills if they get a virus at nursery. The answer is not cognitive – they need to rebuild the knowledge by blunt repetition. Google won’t help.
A new Interoceptive Exposure Therapy may help. IET aims at getting you to read your body and distinguish it’s changes from something that can be fixed by Slow Thinking and concentrating. The problem is therapists doing this may be trying to help people on SSRIs or antipsychotics that are disrupting bodily knowledge – they are trying to put out fires someone else on the team is pouring oil on.
Plateau

To see if SSRIs have an effect other antidepressants don’t have – we randomized 20 health-care staff to 2 weeks of Zoloft or a Norepinephrine inhibitor followed by a crossover to 2 weeks of the other drug. The patients in the unit had no idea this was going on. Carlsson was right. The volunteers picked up a Zoloft reduction in emotional reactivity.
Two volunteers became suicidal on Zoloft – the drug Woody later had. Pfizer did a Zoloft healthy volunteer trial 20 years before Woody had it and concluded Zoloft could cause the agitating effects that killed him.
Two days into our trial, a patient asked me if Doctor X was on a drug – I said yes. I bet it’s an SSRI he said. When we broke the blind he was right. The effects of these drugs good and bad are visible within hours of starting.
Visible to patients who, used to looking at people on these meds, spot effects healthcare staff can’t. You, your family and friends can spot them. But no expert can. The therapist, whose referral got you on meds, can’t see these effects even though we have SSRIs because therapists could once spot this.
Woody knew Zoloft was not suiting him and told his doctor. James Holmes, the Batman Dark Knight Killer told his doctor if you could see the thoughts in my head you’d lock me up. Woody had a good doctor, whose insistance he continue treatment, killed Woody and left his doctor feeling very bad. Telling James Holmes he was responsible for any thoughts in his head, his doctor contributed to killing 12 people and injuring 72 others – in my opinion. I’ve no idea if she finds this difficult to live with.
When I said Peak Experience did you imagine standing on a peak surveying all around you? Peek is what you do from the top of a Big Dip.
Peek Experience

Woody was and you are dealing with Religion not Science. Woody’s doctor, Chris Armstrong, is a decent man. He followed the Good Book and Standards of Care. Religions Follow Truths, sometimes laid down 2000 years ago, or a century ago or in this case 35 years ago. Science starts when we begin a treatment. It is a process that can change what is established from last week to this.
Health has replaced holiness today. Religions though are not about fostering holiness or health, they are about keeping a tribe together. Branding creates tribes – Catholic, Protestant, SSRI and CBT tribes. The Religious once confessed Sins, now we confess our Flaws ADHD, ASD and Trauma and are saved.
Religions tolerate abuses like Sexual Abuse of children and Woody’s Abuse by Drugs because they offer Magic Principles that give our world order.
Health has borrowed two Magic Principles from Catholicism – Sacraments and Infallibility. Sacraments can only do good and cannot harm – just the opposite to Poisons. Transubstantiation converts the Eucharistic bread into the real body and blood of Xt. But Catholics have recently been forced to recognize that gluten remaining in a real body can harm us. the Eucharist is now less of a Sacrament than our meds have become.
RCTs transubstantiate our meds into Sacraments.
This began in 1990, when 3 Boston clinicians reported 6 patients becoming suicidal on Prozac. Twenty groups reported the same thing. In response, Eli Lilly claimed their RCTs showed no evidence Prozac caused suicide. Lilly branded RCTs as the science and branded your and your doctors reports as anecdotes – misinformation.
If a man is on trial for murdering his wife and his lawyer argued he’s innocent because RCTs or epidemiology show that even men with a criminal record, legal and financial problems, and wives no-one liked, on average do not kill their wives – You’d say Give us the specifics of the case and we’ll decide if he murdered her. It’s the same for SSRI suicides and drug hazards.
RCTs give averages. Science and justice are about individuality not averages. specifics not generalities. Like a jury, we need to observe details and come to a consensus that moves us beyond your opinion or mine. We create facts, which can change if new details emerge.
As the average effect of SSRIs in RCTs is weak, some folk claim these drugs are no more than placebo. This plays dangerously into Pharma’s hands. Saying these drugs are placebos means good doctors figure Woody telling them weird things are happening in his head is fantasizing.
This shows the peril of not knowing, in the Biblical sense of knowing, what a drug can do by taking it. If you average paper accounts of good and bad trips on LSD you might claim LSD effects are just placebo.
When SSRIs suit or don’t suit you, you know what’s happening you. But we who should be doing science with you have lost our ability to work with you.
What proportion of SSRI Trips are Good or Bad? Half of company SSRI trials failed to show a benefit – and 1 in 5 people drop out because of neuropsychiatric problems – that’s a lot of bad trips. A proposal to list the negative trials in the Zoloft label was shot down by an FDA eminence grise called Bob Temple.
The remaining trials contained some people who got a benefit so marked it can’t be put down to placebo. The changes for this good trip group let FDA license SSRIs. How big is this group? Less than 1 in 5 of you put on an SSRI will have a good trip. FDA knew this 35 years ago.
I hope no-one has a Near Death Experience at the sight of figures.
Religious Docs claim the Magic of RCTs is they control for all possible confounders. But RCTs don’t control for the main confounder – Our Ignorance. We’re ignorant about Dementia, Diabetes, Parkinson’s, back pain, ASD – superficially similar mixtures of different conditions that show different treatment responses which allow companies to play tricks like these.
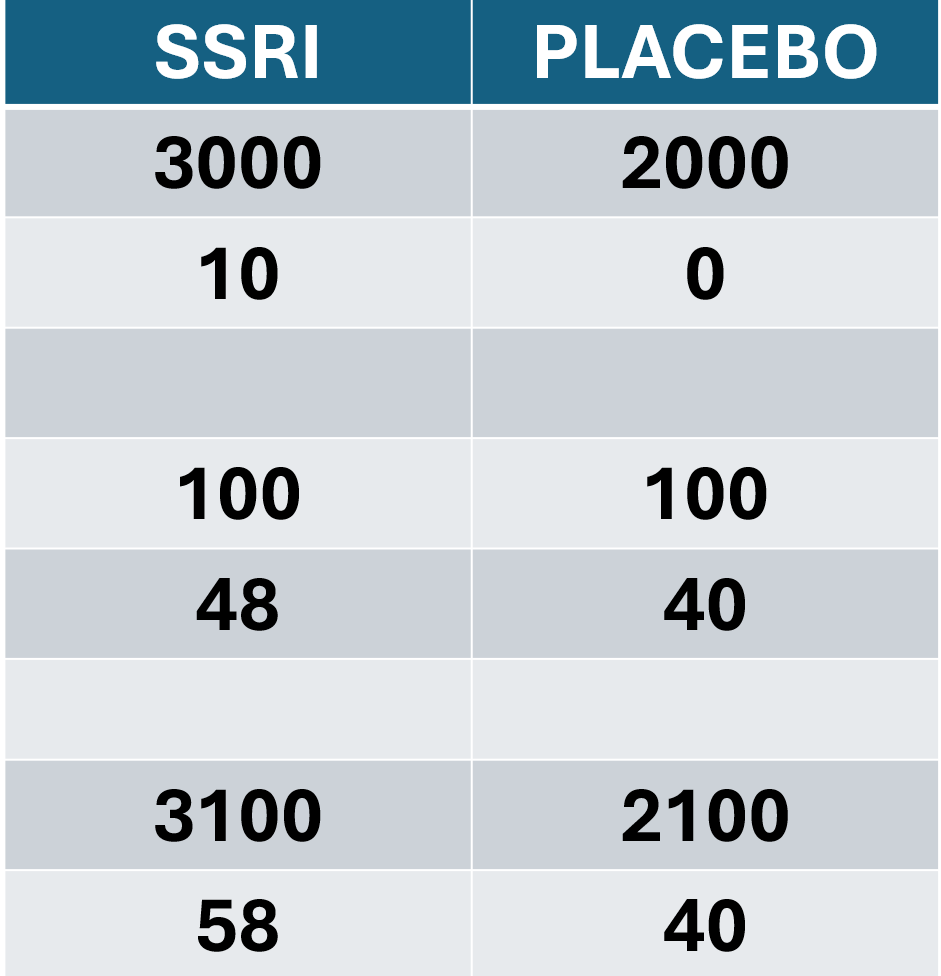
Line 1 shows you the number recruited to trials of Drug A v Placebo and Line 2 the suicidal events on A. No one would take Drug A based on these figures.
Lines 3 and 4 show you the numbers and suicidal events in another trial of A v Placebo. Not so clear but again A looks riskier.
When added together lines 5 and 6 show dangerous Drug A looking safer than Placebo.
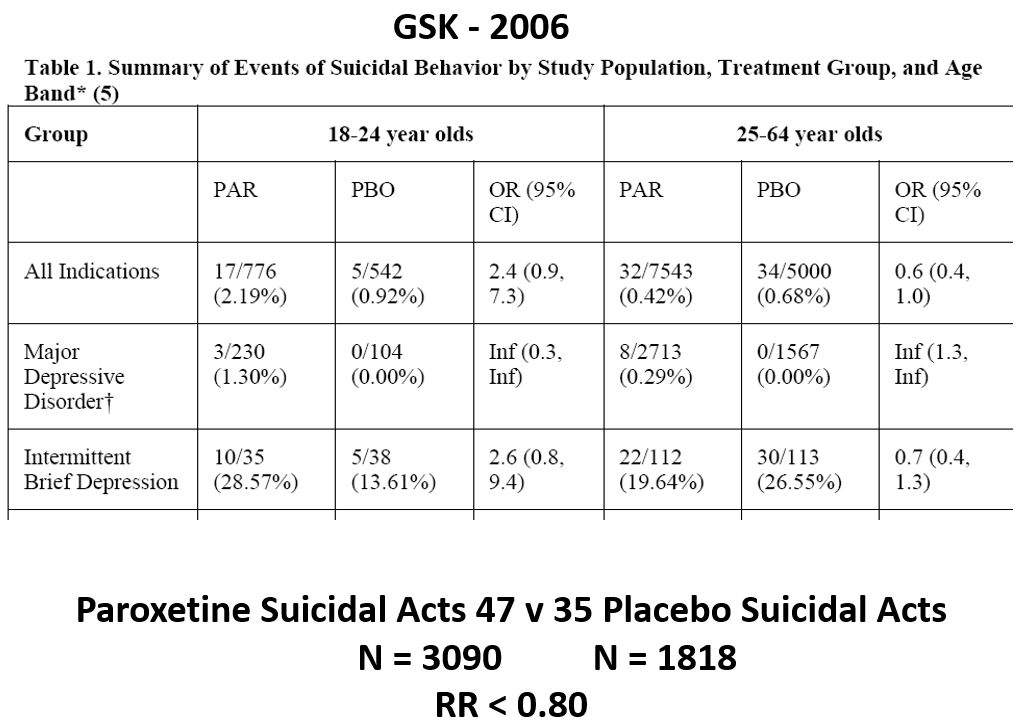
GSK played this trick on FDA. This document shows Paxil trials in MDD and intermittent brief depressive disorder patients all of whom could be recruited to a depression trial. Mix them and bingo Paxil saves lives. I could have advised them to play this game.
Look at the Statistical tests column on the right – these supposedly provide the Infallibility, the Objectivity, your and my subjective consensus cannot provide.
Companies use statistics to claim that unless a 100 barreled gun has 95 bullets in it we kno infallibly it is Not Loaded. Decades back statisticians said this is crazy – Confidence Intervals are better. When poor telescopes 200 years ago left us unsure if we were looking at one or two stars, confidence intervals could manage this ‘instrument error’. But if my heart slows on a beta-blocker and David’s speeds up this is not measurement error.
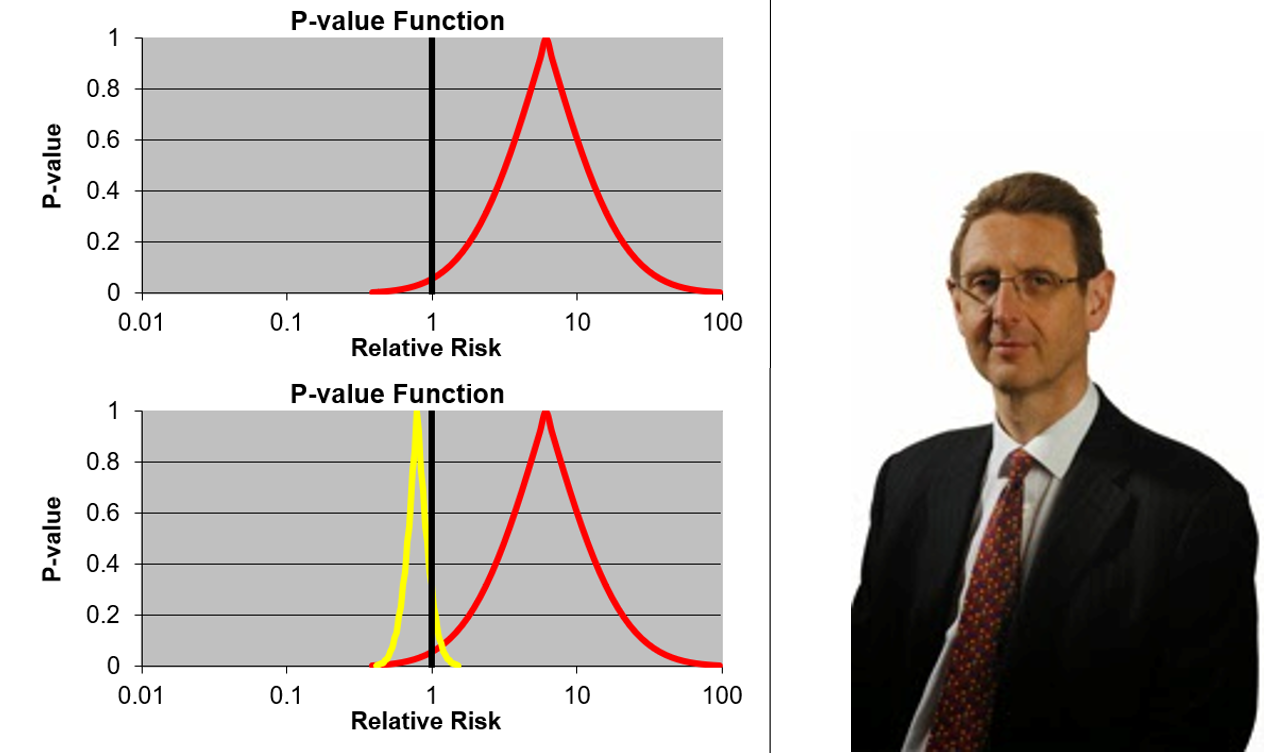
The Red Curve shows you the broad confidence intervals for GSK’s MDD data. Everything to the right of that black line says the gun is loaded. The teeny bit to the left is what GSK use to say its not loaded – there is only 94.5 bullets in this gun.
Confidence curves are meant to tighten up if we add more patients. The expectation is all the data will lie to the right and we should see the gun is loaded.
GSK added a few more patients and we have a much tighter Yellow Curve but on the other side of the 1.0 line. You could leave this gun lying around the house with the safety catch off and your children would be at no risk.
This Slide also shows Cardinal Ian Hudson, GSK’s Chief Safety Officer, testifying at the trial of Don Schell who, like Woody, after a few nights poor sleep, was put on Paxil and 48 hours later shot his wife, daughter, granddaughter and himself. Hudson told the jury GSK practice EBM and RCTs show Paxil has no side effects.
The Jury decided this man did not murder his family. Paxil was loaded and GSK were responsible for these deaths. These statistical tests have no roots in healthcare. They don’t deliver objectivity. The jury decided their consensus was more objective.
For his sins, Cardinal Hudson was later made Pope Ian of the UK’s FDA. To this day, Hudson thinking sits atop our Health Vaticans.
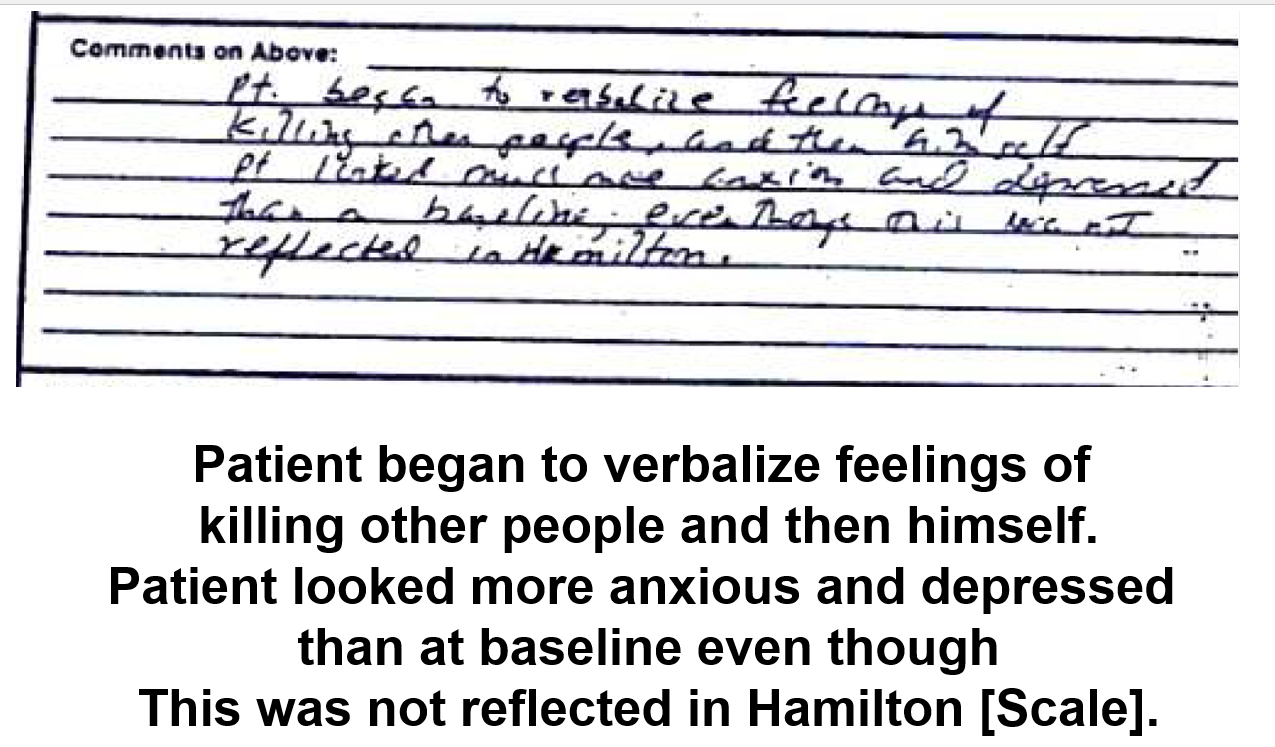
Rating scales and statistical tests inhabit a virtual world. On a Depression rating scale, this man is doing well on Zoloft in a 1983 Pfizer trial but the scale didn’t pick up he is thinking about killing people and then himself. An interview did. A few months earlier than this, Pfizer had seen problems like this happen to healthy volunteers given Zoloft and wrote Zoloft can cause this. This man was removed from the trial, with his withdrawal coded as Nausea. Other Pfizer completed suicides have been coded as burns.
The same week as the Tobin verdict, a prosecutor and judge looking at the case of a man put on Zoloft, after a few nights poor sleep, like Woody, ended up in a state like this and killed his wife, said it’s obvious Zoloft killed her.
But Woody’s doctor couldn’t see this. When Kim told Bob Temple, FDA’s eminence grise, about Woody’s case, lying on the floor besieged by crazy thoughts, Temple responded Woody was an anecdote.
You probably know these are the witches from Macbeth. Macbeth was a Tragedy – that means the central figure has a flaw that is his undoing.
Austin Bradford Hill who created RCTs said they tell doctors nothing about how to treat the patient in front of them – a good interview is better. He added that if we ever thought RCTs were the only way to evaluate a drug we would have gone mad.
Let me paraphrase what he said:
All RCTs are dangerous. They generate Ignorance. Our challenge is to bring some Good out of this.
But companies and regulators now claim RCTs offer Gold Standard Evidence. This claim has transformed a Medicine, which aimed at remedying our health needs, into a Trans Medicine catering to our discontents. It has transformed our drugs into Probity Blockers.
RCTs are the Milk of Paradise.
We are dealing here with what the Ancient Greeks called Rhetoric – the Art of Persuasion. We are not dealing with a Big Pharma making drugs we Need. We have Big Propaganda exploiting our Wants – our First World Discontents – tempting Us..
With the development of AI, the audience here are dealing with not just Big but Total Propaganda, That’s why America and the Rest of Us need you.
We are part of the tragedy and face a War on Science from a Religion whose rallying cry is Science Will Win.
The Witches of Big Propaganda told Macbeth he was safe until Birnam Wood moved to Dunsinane. They tell Lilly and Pfizer they are safe, while we believe in RCT Gold.
Our desperate need for a father figure, lets companies seduce us into delegating our narcissism to FDA, especially once Bob Temple bought into the RCTs are Gold story. Thinking we have a Safety System is tragically Unsafe.
FDA approval is like FAA approval of planes. Pilots not FAA keep you safe in the air. The pilot has an incentive to land and report because if you don’t get to where you’re going she probably won’t either.
Doctors are supposed to keep us safe on a pill but have no such incentive. Doctors have drunk the Milk of Paradise. If you say Hey a door has blown off this healthcare plane you risk being thrown off as a spreader of misinformation. If you’re prescribed a med, get a parachute.
Prescription-only is a police, a surveillance function, that is not needed for 100% effective and safe drugs. Doctors are rapidly being replaced by nurses. They are sleep walking into oblivion. You might be safer with over the counter meds.
We often think market forces or social forces are the only thing that can improve health but the greatest drivers of modern healthcare have been the US military. They don’t need treatments to work in the sense of making more money, they need treatments to give them more and healthier troops but US life expectancy and reproductive rates have fallen below most countries and disability rates increased. Like pilots the military have an incentive to get things right – if they lose out the Chinese military will replace them.
Maybe the military will chop down Birnam Wood, check Dunsinane on Google Maps and head there.
Confronting a sword wielding Macduff, Macbeth said no man of woman born could harm him. He heard MacDuff growl back he was from his mother’s womb untimely ripped.
Macbeth’s efforts to impose order on Scotland killed a small fraction of the number killed by Bob Temple’s efforts to impose order on FDA through his weaponizing of RCTs.
You don’t have to be a man or wield a sword to face down a Bob Temple. Kim confronted Temple and put Woody’s death firmly in his lap. Temple, using a word he knew to be an insult, said Woody’s story was an Anecdote.
Kim response has been: We Are Not Anecdotes.
The Creation of Science
Macbeth was first staged in 1606 at the Globe in London. A mile away, 54 years later, a group of men – they were all men – created Science. They began holding events like transfusing the blood of a young dog into an ill old dog who seemed invigorated. Or looking down what we now call a microscope and seeing tiny animals we would now call microbes, germs.
These Events – Case Conferences – produced Observables. Like a jury, the witnesses were challenged to come to a consensus on what they saw.
A Case Report – which industry and Bob Temple brand Anecdotes – was made for the event and its consensus. This process is what put men on the moon, decoded the human genome and extended life expectancies.
Medical journals came 200 years later. RCTs and their statistics came 300 years later. The 1950s was the stellar decade for drug discovery with almost all classes of medicine we now recognize coming into being. None of these breakthroughs involved RCTs. Many of these drugs, like imipramine, remain far better than treatments like the SSRIs we have today. The SSRIs are useful primarily for the extra option they offer, not because they are generally good or safe.
Let’s take Woody into this 1660s room. Kim who saw the change in him would also be there. Woody’s mother who later told Kim Woody was worried about harming her should be there. Dr Chris Armstrong, who started the experiment by putting Woody on Zoloft is there. Ideally someone doing well on Zoloft will be there. Someone from Pfizer too – who said 40 years ago Zoloft can do this. Bob Temple should be there too. What will the consensus be?
This is the purest form of science there is. The Rules would say no Zoloft RCT can be brought into the room. Why? We don’t have access to the man coded with Nausea or the man coded as Burns or any people in these trials. Company studies are Hearsay, not Observables, not Evidence.
Chris Armstrong was horrified by what happened to Woody. Let’s say though he said as many good therapists and doctors would – hey look I’m not a scientist, I’m in this because I care for people.
if I were Woody or Kim my response would be – If you’re not able to engage with me, and I don’t mean persuade me to believe some Truth you held before I came into this room, I cannot see how you can Care for me.
Let me show you how far we have drifted from Science. If we write up a Consensus Report on the outcome, as things stand, medical journals would refuse to publish. It is only when out leading journals publish reports on a case like Woody’s that I will feel confident that Birnam Wood has arrived at Dunsinane.
Some Water needs to accidentally fall on these journal editors – these Witches from the West.
Ghosts in the Machine
Clearly this is Science and Woody’s ghost is not about to appear in the room the way Hamlet’s father did. But if like Hamlet’s father, Woody’s ghost told you he had been poisoned by someone expected to be on his side, while he was lying down – the poison was not put in his mouth – it was poured into his ear, how would you respond?
Hamlet promised on swift wings to sweep to his revenge. But he ended up agonising saying:
The time is out of joint. O cursed spite
That ever I was born to put it right

That indecision was Hamlet’s flaw, his tragedy. It is also our story.
This from Reno made me feel terribly sad. This is a magnificent portrayal of the before and afterlife.
No-one knows better, than David and Kim.
Did they receive a standing ovation. Did the audience understand the years of meticulous work that went in to this. Did it make them think. Did it make them care.
Do you think airline pilots care about their passengers? They do, but not in the way you think they do. I have spent a lifetime with airline pilots. I went to a funeral recently of a retired airline pilot. All the pilots attending had stories ‘they took an engine from a different plane and put it in his plane in Africa and a small boy cried ‘man hanging in tree’.
Pilots have a passion for planes, from small boys, they wanted to fly large and small aircraft. Get a group of pilots together and the conversation will not stop comparing aircraft, experiences and near misses.
Doctors are a different breed. I doubt you will ever hear, ‘that was a close call, my patient nearly died from an SSRI’.
Professing to care, pretending they know what they don’t know, and and being the ‘first port of call’ is a ‘tragedy waiting to happen.
Thanks for the Rapid Report from Reno, and a special thanks go to Kim for her superhuman strengths starting with the loss of Woody..
It was a care-crash.
Very powerful and deeply moving post. Thank you.
As hard-hitting a talk as you promised. And viscerally moving – thanks to Kim and Woody’s presence. Important that Zoomers were in the audience, since the riskscape for their generation seems the most confused – and alarming.
Bill Maher quoted some 2024 figures from the Skeptic Research Centre (SRC) – putting numbers on what we can all clearly see. Amongst Zoomers, 73% of women and 67% of men believe that ‘mental health challenges are an important part of their IDENTITY’. Amongst Boomers the proportions are reversed.
Celebrated American actor/tress, Kristen Bell recently described explaining her ‘mental health meds’ to her children as, ‘It’s BROCOLI for my brain’.
https://www.today.com/parents/moms/kristen-bell-mental-health-rcna63938
Why does almost nobody join the dots – the rate of initiating antidepressants, as you often observe, is growing fastest amongst young women. The suicide rate is also growing fastest amongst young women.
You drew my attention to Danny Blanchflower’s analysis of the declining ‘mental health’ of the young – or growing ‘ill-being’ as they call it – across 160 odd countries. They see the patterns but don’t seem to join the dots either:
-deterioration in mental health is a major cause of increasing hospital admissions among young people
-higher rates of depression result in higher usage of anti-depressant drugs suggesting self-reports are accurate.
-declining mental health has been linked to rising suicide rates, especially among the young
Yes, yes and yes. But what about causes – job market repercussions from the 2008 recession, depletion of healthcare resources and the inexorable rise of smart phone technologies and their socio-psychological adverse effects.
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0327858
Hang on, Danny, what about the life limiting (SD, PSSD etc.) and life ending effects of the ‘broccoli’? They just don’t see it – which is perhaps why economists are not best placed to understand the ill-being of young women. And why you and Rxisk are.
A REALLY important point made here: that SSRI’s are “useless in severe cases.” (And that SSRI users, like CBT users, are most likely to report improvement if their initial symptoms were NOT severe.)
This is such a critical point, because it’s diametrically opposed to the conventional wisdom regarded by most as “What the Science Says.” At least in the USA.
Both doctors and journalists (even those who count themselves as “medical skeptics”) often state SSRI’s are likely overused in mild to moderate cases–although of course they are vitally important in severe cases!
What’s the main evidence you would offer to refute this doctrine? Are there published studies – or studies that were never published? Maybe even studies done prior to licensing of SSRI’s for depression? Or is it mainly based on overwhelming weight of clinical experience? Any answers worth their weight in gold!
(PS: it often seems to me that the most disastrous reactions, (such as the suicides of Woody Witczak, Stu Dolin and others whose grieving families took drug cos to court), happen precisely in people with relatively mild symptoms from job stress or whatever, rather than serious depression. Does that make sense?)
Jo
Right from the start SSRIs were recognized to be useless in hospitalizised depressive disorders. The studies had to be run in mild depression (really anxiety states) because they did not work in melancholia or anything severe. This was so clear that the companies opted not to run trials in this group. And in trials where SSRIs were compared to tricyclic antidepressants, the TCAs invariably beat them.
The idea that they work in severe depression is because you can just about show they do something sometimes when the Hamilton Depression Rating Scores are slightly higher than in the group who respond to placebo.
The Good Trip (the right amount of emotional muting – and this suits me) and the Bad Trip (agitation or too much emotional numbing or emotional muting but this is not something that works for me) can all happen and at level from healthy volunteers up to patient levels.
David
One of the things that got me in a psych ‘hospital’ was the lack of any creativity. Psychiatrists seemed devoid of it.
Time and again David uses analogy in a cinematic way. Sometimes I’m thinking Fellini as with this one, sometimes Antonioni, Bertolucci or Orson Wells. A massive big dipper ride is a good visual cinematic description of the akathisia Woody, myself and god knows how many thousands of others suffered.
I did a AI chat on akathisia full of info based on current practice to treat akathisia (which makes it worse) and zero creativity.
BTW is there any video of this I can bookmark?
Chris
There is a video up at the top of the post. Hopefully there will be another from the actual meeting
David
“It is a doctor’s practise”
There is so much to this OTC, over the counter.
All these drugs, which Pharma, and doctors, say are ‘safe and effective’, and downplay risks of adverse effects and violence and suicide because of RCTs, in which the positive trials out-paced the negative trials, which weren’t published, and suicides occurred in the negative trials.
If Woody, Tom Kingston, Stewart Dolin, and the legions of others, noticed what was going on, and they did, they would have thought. This isn’t for me, I don’t think I want it.
If they are too hot to handle by patients, and the doctors are giving spurious advice, fed to them by Pharma, why is the safety profile so high?
The safety profile is so well-known, that APA, RCP, RCGP, MHRA, NICE, Etc. promise everyone that no harm will come to them.
Well, obviously, harm has come to them.
The state of Akathisia leads to a state of mind that can not and should not be minimised. This state of mind is what leads to the state that Woody experienced. It is so powerful there is no way out. Killing yourself is the only way to stop it.
It is total nonsense for doctors to say that it is your underlying condition coming back or you are resistant.
Kennedy and Makary and their team, could do worse than than making SSRIs OTC. Would all hell let loose? Would this be considered outrageous? Would there be a total ambush by the organizations above?
Let’s not beat about the bush.
OTC
But what if patient goes back to the chemist and says I feel more agitated on these and the chemist says they take a few weeks to kick in…. Akathisia can happen very quickly and be intensely horrific and nothing can be done about the tablet you took three hours ago in the lull of the agitation. The lull must have been the drug I took yesterday doing it’s job so I’ll take another one and you find yourself in a dipper with no way out.
Chris
If you guy a drug over the counter you don’t go back to a pharmacist to ask what is happening to you. You are much more likely to just stop and the label of the drugs will endorse this.
The idea these drugs take weeks to work is a myth – freed from pre-programmed doctors people will be able to employ common sense in looking after themselves. You will be able to listen to your friends and family when they report what they are noticing in you without doctors telling them and you to pay no heed to what you are noticing.
Akathisia is not the only issue to which this applies. There are many many problems these drugs can cause which can be avoided other than just akathisia
David
As a very sensible man once said to me “no one will know what you are talking about”.
It is difficult to look past the history of science and not acknowledge that the diseases of internal medicine were discovered and validated using simple empirical methods. Dropsy may have contained few natural kinds, but it did have a tendency to cause people to drop dead. You only need look at EDS to see that, had internal medicine not had a head start, the winds of the Enlightenment would likely not have carried it any further than psychiatry.
Case in point, as you rightly point out: “the moon landing”.
Moonshot: Inside Pfizer’s Nine-month Race to Make the Impossible Possible
by Albert Bourl
17 Mar 2022
Albert Bourla reposted
Rapid Response 47@RapidResponse47
.
@Pfizer CEO@AlbertBourla: The big winner of this deal clearly will be the American patient — there’s no doubt about it. They are the ones that will see significant impact in their ability to buy medicines… We are ready to UNLEASH our investment portfolio in this country
https://x.com/RapidResponse47/status/1973062219211354327
The American Patient – UNLEASHED
Britain needs to reverse its declining investment in medicines, science minister Patrick Vallance said on Tuesday, amid growing concerns about the country’s attractiveness to pharmaceutical companies.
UK pharma investment crisis: Why Big Pharma is pulling billions from the UK
https://www.openaccessgovernment.org/uk-pharma-investment-crisis-why-big-pharma-is-pulling-billions-from-the-uk/198340/
Robert clearly doesn’t take truck with Albert, judging by his expression, and Donald, has that face, ‘hmmm, we’ll see’. Patrick Vallance, meanwhile, thinks he still works for GSK.
Take us to the moon
Something’s got to give in the UK NHS – ofc, as you’ve often mentioned, it’s primarily driven by money. All three political parties have looked at the disability bill – in horror.
‘..
.’The prevalence of depression has shot up from 5.8 per cent in
2012 to 13.2 per cent a decade later in 20228. But the rise in need for mental health
services is not evenly distributed in the population. For adults, mental health
referrals have been increasing at a rate of 3.3 per cent a year9. But for children and
young people, the rate of referrals has increased by 11.7 per cent a year from
around 40,000 a month in 2016 to almost 120,000 a month in 202410. And referrals
for perinatal services for mothers has risen by 23 per cent a year since 2016, rising
from around 1,400 a month in 2016 to more than 7,600 a month in 202411’
https://assets.publishing.service.gov.uk/media/66f42ae630536cb92748271f/Lord-Darzi-Independent-Investigation-of-the-National-Health-Service-in-England-Updated-25-September.pdf
So much for the effectiveness of the 90’s ‘Defeat Depression ‘Campaign for human health. A marketing triumph ofc.
It will be interesting to see how politicians de-escalate the epidemic they helped
to fuel.. Carl Heneghan a policy influencer up to a point, said this the other day ‘A large number of people have been medicalised and, as a resul are now taking antidepressants even though these medications show little or no effectiveness for mild depression’. That old chestnut – and no mention of deprescribing hazards.
And profit-centric Wes Streeting, Britain’s Minister for Health, has appointed Simon Wessely to play a lead role as Vice Chair in this – ‘’Labour is launching a review to decide whether some mental health and neurodivergence issues are being over-diagnosed. ‘
https://www.benefitsandwork.co.uk/news/controversial-professor-to-investigate-overdiagnosis-of-mental-health-and-neurodivergence-for-labour
This feels like another cover-up in the making. I’ve finally got my teeth into Andrew Marriott’s ‘If you wake at midnight- the Lariam wonder drug scandal’. Impossible to ever trust the system again.
‘The state of Akathisia leads to a state of mind that can not and should not be minimised. This state of mind is what leads to the state that Woody experienced. It is so powerful there is no way out. Killing yourself is the only way to stop it.’
I deal with this in my mind every day in the very real knowledge that if it happens to me a third time I maywell not survive it. I believe it is possible to stop akathisia ( my view it’s the overwhelming issue that is killing people in and out of psych ‘hospitals’ ) but only at the very beginning or the prelude which is usually emotional lability lower level agitation or at least it was in my case for the first hour or so. You have to do the right things very quickly and consistently and that includes stopping foods herbs and spices that inhibit the drug metabolising enzyems for long after you feel better otherwise it returns and I know, David, you don’t go along with the CYP450 stuff. But it’s my experience trying to save my life not an intellectual exercise. I do not believe the majority of people who have early onset akathisia from OTC would not have any clue how to save themselves, in many cases just stopping is not enough they are more likely to go very quickly to A&E as I did and get a mental health label more drugs and descend into akathisia hell because the medics are also clueless as to what is happening and want the person who has been driving them crazy pacing up and down in a state of terror for hours out of the way. After a certain amount of time they’ve had enough and want them gone and they don’t care if it’s a psych hell hole.
Chris
I’ve no doubt that what you outline here happens and happens a lot and kills people. Part of the problem is that prescription only SSRIs were brought on the market at crazily toxic doses – anything from 4 to 10 times the dose they needed to be in order to achieve the benefits that can be achieved for some. The OTC SSRIs are at lower doses and this is partly why they don’t cause the problems they have the potential to cause.
Plus you are less likely to be gaslit. Go to A & E and say you are feeling bad after an OTC med you took and the system will agree totally that OTC meds can cause this and you will be okay pretty soon. This is completely the opposite experience to the what happens when you say you are on a prescription only med when the you have to keep taking this mantra kicks in.
D
Understatement of ‘The Big Dipper’
Expression of Concern
Efficacy of Paroxetine in the Treatment of Adolescent Major Depression: A Randomized, Controlled Trial (J Am Acad Child Adolesc Psychiatry, 40(7):762-772; https://doi.org/10.1097/00004583-200107000-00010)
https://www.jaacap.org/article/S0890-8567(25)02107-0/fulltext
The Journal of the American Academy of Child and Adolescent Psychiatry is publishing this expression of concern in order to alert readers to concerns that have been raised about the article.
Review of such issues are managed by the journal according to Committee on Publication Ethics (COPE) recommendations and guidance.
Further review is underway, and an expression of concern will continue to be associated with the article until an outcome is reached.
Accepted February 15, 2001.
https://study329.org/wp-content/uploads/2015/02/Keller-et-al-329.pdf
Accepted 3 August 2015
https://www.bmj.com/content/351/bmj.h4320
The RIAT researchers identified Study 329 as an example of a misreported trial in need of restoration. The article by Keller and colleagues, which was largely ghostwritten,3 claimed efficacy and safety for paroxetine that was at odds with the data.4 This is problematic because the article has been influential in the literature supporting the use of antidepressants in adolescents.5
In later correspondence, GSK stated that the study by Keller and colleagues “accurately reflects the honestly-held views of the clinical investigator authors” and that GSK did “not agree that the article is false, fraudulent or misleading.”6
As with most scientific papers, Keller and colleagues convey an impression that “the data have spoken.” This authoritative stance is possible only in the absence of access to the data. When the data become accessible to others, it becomes clear that scientific authorship is provisional rather than authoritative.
Healy and his co-authors write:
The question for every reader is: How could a journalist with no medical training, Shelley Jofre, spot the problems that the authors and reviewers of Study 329 failed to detect? Precisely because she was not in the field, the journal’s reputation and the distinction of the names on the authorship line meant nothing to her. Because statistical significance was not part of her everyday world, she wasn’t hypnotized into thinking that non-significant events weren’t happening. She didn’t assume ‘emotional lability’ referred to some inconsequential change on treatment; she noticed that it was happening more on Paxil and began to ask questions. The lack of sensible answers ultimately led to the discovery of company documents conceding that Paxil didn’t work and that the entire study was ghostwritten. (p 87)
The editor of the New England Journal of Medicine, Jeffrey Drazen, even suggested that the re-analysis of studies would produce a new breed of “research parasites” who published papers based on the work of others, thereby throwing cold water on the idea that communal access to clinical trial data could serve the scientific good (8).
The lessons of Study 329: How fraud in psychiatric drug research got normalised
August 29, 2020 by David Healy 1 Comment
https://samizdathealth.org/the-lessons-of-study-329-how-fraud-in-psychiatric-drug-research-got-normalised/
Annie
Thanks for this. Its an important reminder of the issues at stake and how far mainstream medicine has drifted off course and how journals are actively complicit in working with pharma to the detriment of all of us.
Some of us figured two decades ago it was time to sue our journals, maybe Skip Murgatroyd’s initiative to sue JAACAP might open the door to something like this – I imagine everyone (including me) except those who have injured by these medicines will shudder at this thought. We need a Hercules to clear out a bunch of Augean Stables.
D