
The Back Story
Britain’s Royal College of Psychiatrists recently produced a book, Mind State and Society, edited by George Ikkos and Nick Bouras. MSS celebrates 50 years of psychiatry during the period 1960 – 2010.
George approached me for a chapter on pharmaceutical industry input to the period. I wrote The Pharmaceutical Industry and the Standardisation of Psychiatric Practice. This chapter pulled no punches. I was pleased when George and Nick left it intact and indeed seemed to think it was quite good.
On October 5, my mother’s birthday, and the day of Frances Haugen’s testimony to Congress about Facebook, a meeting was held in the Royal Society of Medicine (RSM), featuring a day of talks from contributors to the book. The talks were recorded. Afterwards, I made several requests to the RSM for a copy of my talk in a form I could upload, without a reply – at this stage unaware of the closing comments.
I Zoomed in for the early afternoon session in which I was participating and missed the closing comments from Tom Burns, author of Our Necessary Shadow, The Nature and Meaning of Psychiatry – very much an establishment take on psychiatry.
Getting nowhere with the RSM, with the help of Bill James, I home recorded the talk on Zoom, in the same room, wearing the same clothes – see October 16 Presentation.. No two presentations however can be identical and neither map straight onto the text below.
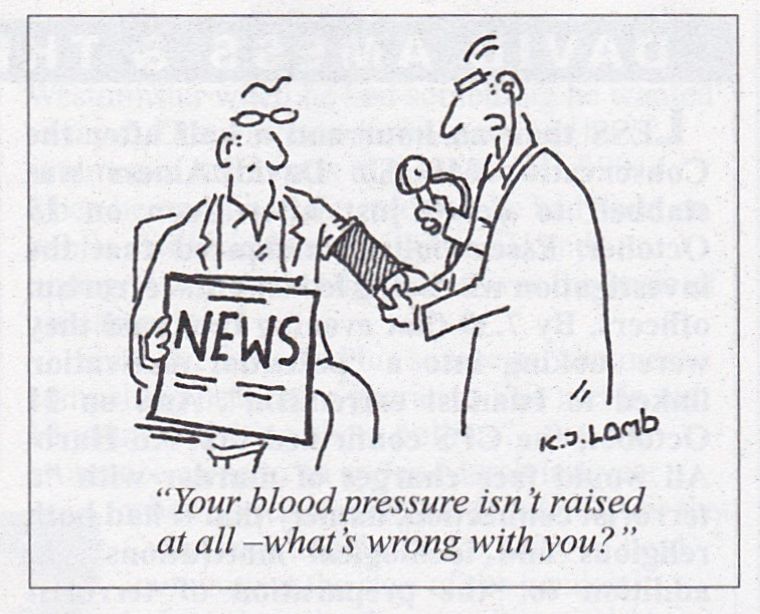
TB’s advice to any doctor tuning in to the lecture is to check your blood pressure before and during as you, like he, despite the occasional useful point, are likely to fume.
Maybe Tom’s been fuming for 8 years. I reviewed Our Necessary Shadow when it came out – See The Nature and Meaning of Psychiatry.
Slide

Psychiatry has often been viewed as a backwater not the leading edge of medicine. This is odd in that psychiatry was the first medical speciality, the first to have its own hospitals, the first to have its own journals, and later the first to turn to community care.
More recently it has been the first to developments in the realm of industrialization and standardization – up to 1990 no one would have predicted its lead in these areas.
Around 1960 British psychiatry was flourishing in part because German psychiatry emerged disastrously from WW II and American psychiatry took a detour into Freud and psychobabble, leaving British psychiatrists as magisterial figures on the world stage.
Slide 3
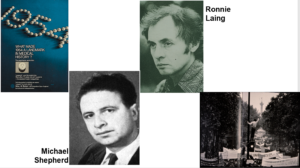
1954 saw the arrival of chlorpromazine in Britain. The first RCTs of psychotropic drugs were done in Britain. Michael Shepherd whom you see here was the leading advocate of RCTs but later ended up with doubts about them. Laing was the face of antipsychiatry, which had a prominent home in the UK.
The tensions between new techniques like drugs and RCTs – were they enhancing or diminishing us – burst out onto the streets in1968. This is Paris – the students marched among other places to Jean Delay’s office – the discoverer of chlorpromazine and ransacked it. Where psychiatrists saw liberation from the shackles of illness, many saw a shackling by drugs.
These 1968 scenes look like something replaying again 50 years later.
Slide 4
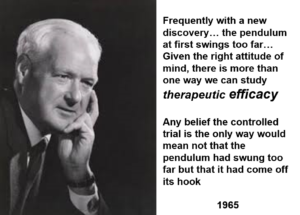
Here you see Tony Hill who ran the first RCT – of streptomycin in TB. This found out less about streptomycin than a standard clinical trial two years earlier. No-one did RCTs for nearly 20 years after Hill’s – until an event – the birth defects caused by thalidomide – led to their incorporation into the 1962 US Food and Drugs Act.
Hill mentions in a 1965 lecture from which this quote comes that to his surprise the people who were most enthusiastically drawing doctors attention to RCTs were pharmaceutical company people.
This quote makes another point clear – RCTs have a place in evaluation but they are not a good way to evaluate a drug. They focus on one thing a drug does when many drugs have several thousand effects.
RCTs do, however, replace clinical judgements with operations. Their incorporation into the 1962 Food and Drugs Act was a key act in the standardization of medicine.
Slide 5
When Tony Hill ran RCTs on antibiotics the endpoint was saving lives or getting people back to work – and you can run a health service for free if you most of what you do meets these goals.
But in psychiatry as in many areas of medicines, RCTs often have more dead bodies in the active treatment arm than on placebo. Working in trials means an effect on a surrogate outcome which in the mental health arena means rating scales – the most famous of which is the HAMD.
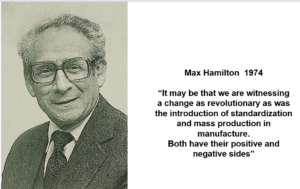
Here you see Max Hamilton picking out a key consequence of the use of checklists. His view was they were prompts to help an interview – not a replacement for an interview.
But checklists risk standardizing the interactions between people, and rather than us helping people to live the lives they want to live, we end up helping them live the lives Pfizer would have them live.
Slide 6
As slide 6, which you see here, brings home.
Slide 7
Through to 1980, the pharmaceutical industry was seen as a good thing. In 1968 people were afraid of Big Medicine not Big Pharma.
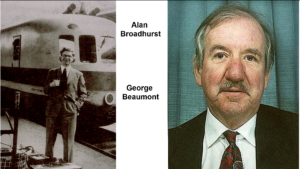
Alan Broadhurst on the left here working in Geigy did a huge amount to get depression recognised and antidepressants used – he probably compiled the HAMD checklist.
George Beaumont, also from Geigy, played a similar role for OCD and clomipramine.
What they did would be called disease mongering now but was viewed as educational then.
Slide 8
Clinicians, meanwhile, recognised the adverse effects of treatment in a way they are unable to do now. Even though we largely viewed the antipsychotics as an extraordinary boon, like Covid vaccines now, doctors were able to recognise problems like Tardive Dyskinesia – even in patients on backwards who were unable to advocate for themselves.
Now we have equivalent syndromes, like PSSD or protracted withdrawal syndromes, affecting thousands of people with great media contacts but these conditions remain invisible now because we – doctors – get in the way.
Slide 9

Our apparent core business at this point was schizophrenia. Schizophrenia has been vanishing – there are much fewer cases than before. We show no interest in this disappearance – just as classic postpartum psychosis has all but vanished with mother and baby units closed all around the country without anyone wondering why.
Maybe our core business is not what we thought it was.
Slide 10
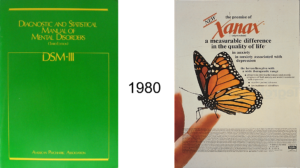
Around 1980, all changed. DSM III emerged. In the UK, before 1990 we paid little heed to DSM except to note a strange new illness we’d never heard of before – Panic Disorder. Was it real – or were the Americans just catching up with something we called by a different name?
Was it really Upjohn disorder – coined to market Xanax?
Some of us began to hear about operationalism for the first time. It had a basis in the philosophy of science – names like Carl Hempel were bandied around. DSM brought an explicit operationalism to the fore. A check-listing. A standardization.
Slide 11
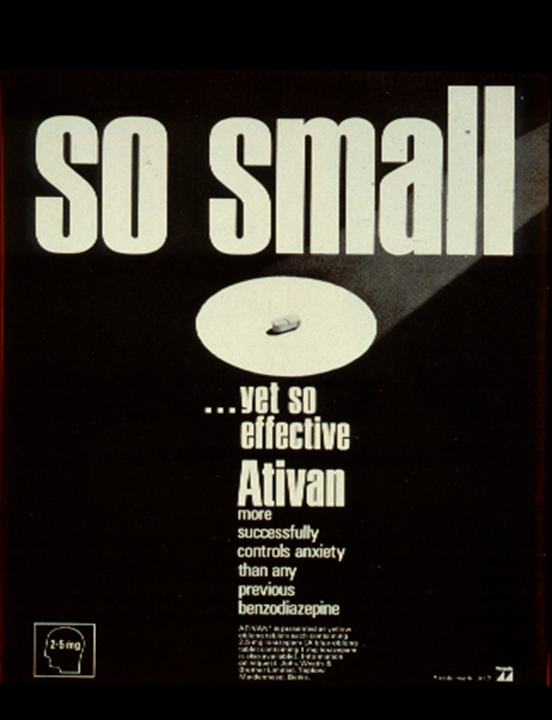
Meanwhile pharma which had been small began to get Big and intrude into our lives. When a crisis blew up about the benzodiazepines, Pharma were in the frame.
This crisis had a superficial continuity with antipsychiatry but Pillars of the Establishment sided with patients who were ordinary people rather than people marching to change the world order.
Slide 12

The Benzodiazepine crisis brought the media into health. The benzodiazepines could never have become the crisis they were, were it not for That’s Life, which you see here.
Before 1980 health rarely featured in the news, aside from standout events like Heart Transplants but now we got health pages, and health on the front page – sometimes occupying more than one slot on front pages. All of Health, not just Mental Health was en route to taking the place religion and politics had previously had.
The work Risk had featured in the Titles of Abstracts of less than 200 papers up to 1970 – by 1990 it had featured 20,000 times. Medicine – or rather pharmaceutical companies discovered risk before Ulrick Beck mentioned Risk Societies.
And where an increased awareness of man-made risks led to a Green movement and a push-back against chemicals and nuclear power – in health it led to just the opposite – an increased consumption of chemicals.
Slide 13

In just the same way as medicine discovered risk before the wider culture did, so also medicine discovered the operationalism and hypnosis by metrics that we now call neo-liberalism. Thatcher and Reagan followed the 1976 introduction of operationalism into what became DSM III.
The idea of the money-supply then and the inflation target appeared – something politicians could focus on to treat the economy or the country and be praised for doing even if the country fell apart as a result.
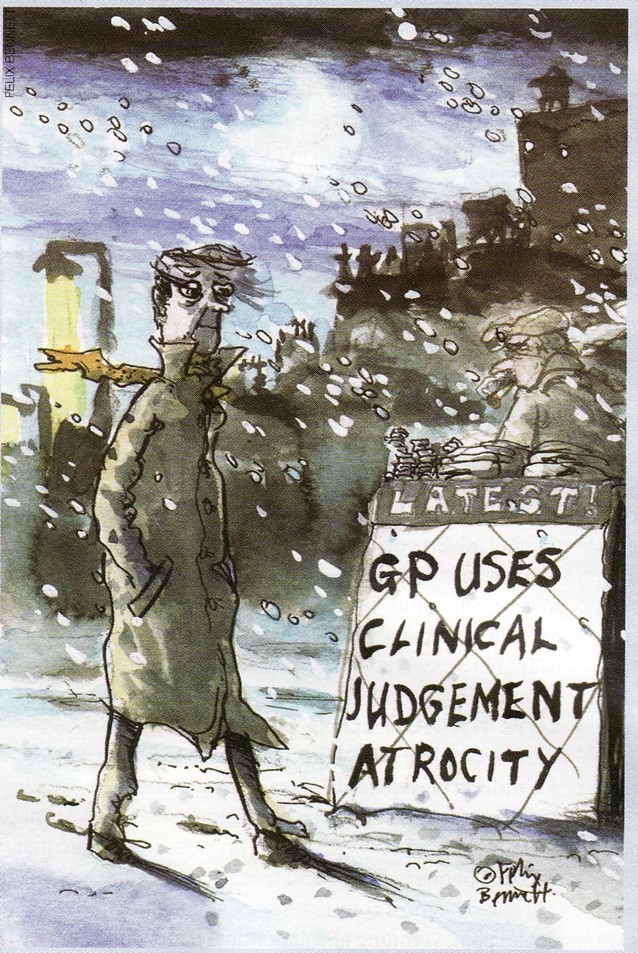
This followed behind medicines turn to treating Blood Pressure, Blood Sugar, Peak Flow Rates or Rating Scales numbers – all of which call for the use of a pill which we can be praised for prescribing, indeed will be penalized for not prescribing even when it’s a disaster for the patient for us to do so.
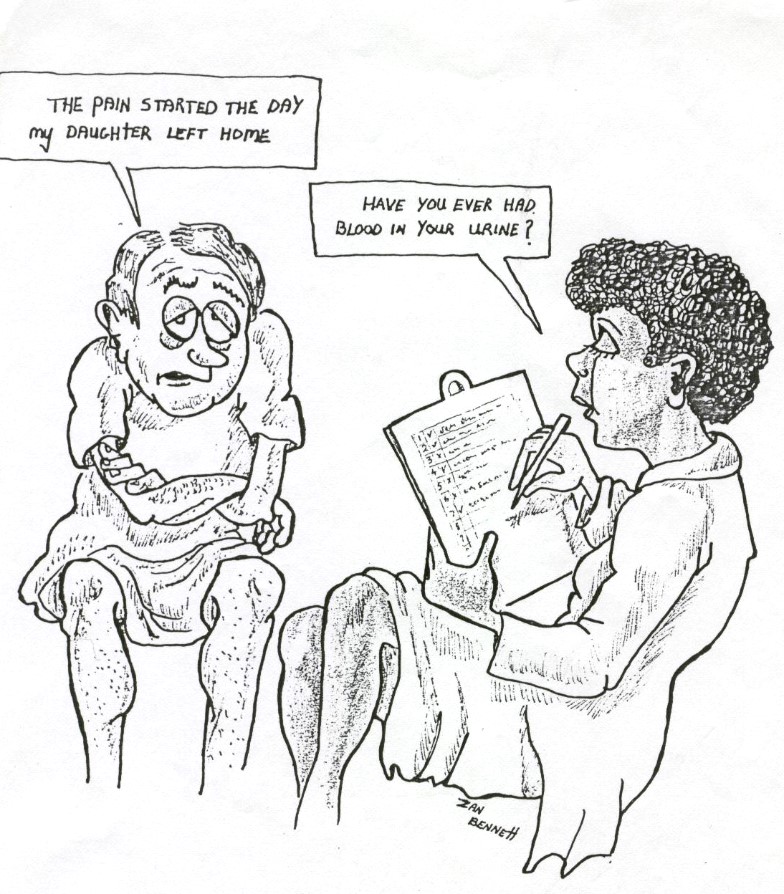
Slide 14
We can see the dead hand of measurement and targets in these two images – management are certain that checking lists has to be more objective and scientific than being present with someone. Two thousand years ago, the Greeks could see how foolish this might be.
Slide 15
Behind the scenes, Pharma was stirring.
They played a significant part in bringing down the benzodiazepines – which were off patent and worthless – in favour of non-dependence producing antidepressants. Britain was about to switch from being anxious or tense and having nervous breakdowns, to being depressed – a low serotonin people as this Guardian article suggested.
Slide 16
In the late-1980s, the NHS began to outsource services like cleaning staff in response to the suggestions of management consultants.
The years before that, in the mid-1970s, in response to the suggestions of management consultants, the pharmaceutical industry had outsourced the running of clinical trials to Contract Research Organizations, now a $40 billion business and the writing up of clinical trials to medical writing companies – ghost-writers.
CROs are the ones who code and collate the figures collected in trials passing them on to the ghostwriters. No one gets to see the data – not FDA, MHRA, NICE or anyone.
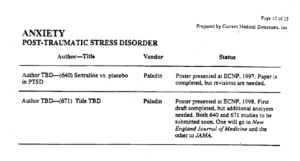
This slide is from a document produced by a company co-ordinating the ghostwriting of articles on Zoloft for Pfizer – see Cattell for more. You see on the right – 2 PTSD articles have been written and the company knows where these will go – to the very best journals in the field. None of these journals are bothered about whether the patients actually exist or whether the claim that the drug works is valid or not. None ask to see the data.
On the left you see TBD – To Be Determined. The ultimate authors need not be people who ran the experiment. Neither these authors, nor the people who ran the study, nor the ghostwriters have access to the data in the trial. The authors will be the people who Pfizer marketing think will do the best job selling Zoloft.
Slide 17
Just like Tony Hill was surprised to find drug companies promoting RCTs – in the 1990s drug companies strongly supported a new kid on the block Evidence Based Medicine (EBM). Doctors meanwhile thought EBM was a way to control pharma, like they had once viewed RCTs.
Doctors don’t now have obvious pharma people in their office giving them free lunches, or if they do these reps will encourage doctors to be evidence based. Pharma now have totally independent groups writing guidelines to sell medicines for them – like the National Institute for Healthcare and Clinical Excellence (NICE). And medical job contracts increasingly mandate that we adhere to these guidelines.
Where drugs are concerned, these guidelines are based on a ghostwritten literature. The people who write them have no access to the data from any of the trials they cite as evidence in support of what you or I are supposed to do. Guidelines only talk about the Benefits of treatment – not the Hazards.
I have written to the Chair and CEO of the NICE guidelines in the UK, regulators in the UK and Europe, politicians and others and none of them deny these points. Their response is one that I have given them – that it’s not their job to police the medical literature. See Crack of Doom.
All of the correspondence is available on the Politics of Care Forum on dhblog.wpengine.com
Slide 18

There are some key dates in the transition away from What Used to be Called Medicine to the health service jobs most of us have now. One date was September 20, 1991 – almost exactly 30 years ago. All through the year before, there were convincing reports of people given Prozac, becoming suicidal, with the problem clearing when Prozac was stopped, and reappearing when it was restarted. See Let Them Eat Prozac.
FDA were forced to have a hearing on antidepressants and suicide. Eli Lilly pitched their RCTs in response stating:
- the plural of anecdote is not data
- it’s the disease not the drug
- are you going to believe the anecdotes or the science?
On the day of the FDA meeting, the BMJ, the most pro EBM medical journal, published Lilly’s meta-analysis of its RCTs, which claimed to show no increased suicide risk.
The article shows an increased number of suicidal events on Prozac – but in the main paper this was not statistically significant which meant BMJ were happy with a statement that the problem didn’t exist. BMJ must not have read the small print in a footnote of the article they published which contained an admission about an ‘illegal’ coding of one event. Reverse this and the suicidal events were statistically significant.
FDA talked about heart-breaking cases reported to them but concluded the science didn’t support the drug causing the problem. FDA meanwhile were sitting on data for sertraline and paroxetine showing the same limited efficacy compared with older antidepressants, like imipramine, and increased suicidal event rates on all three SSRIs with Lilly, Pfizer and SmithKline breaching FDA regulations to hide the problems.
FDA opted not to warn because warning would put people off seeking the benefit – from a treatment that according to them had a favourable benefit-risk ratio even though more people were dying on the active treatment than on placebo.
From this point on the hazards of drugs began to vanish. Journals like the BMJ became scared to take case reports which previously had been the bedrock of medicine. Drugs and Therapeutics Bulletins vanished – replaced by Guidelines which only listed benefits.
Doctors have now lost a sense for drug induced toxicity which is often coloured by anxiety or depressive symptoms. There are no treatments licensed for toxicity and so faced with someone saying they feel anxious or depressed as you can do when you have the Flu, are pregnant, or have a toxic reaction to a drug, doctors increasingly give more of the drugs that are causing the problems in the case of psychotropic meds.
As a result, Patients have become Invisible. We don’t hear or see them in the way we used to.
If patients become invisible, we do too. Managers don’t see or hear us dealing with toxicities that need expert input. Managers see drugs that the evidence says work well and are free of problems and figure doctors can be replaced with cheaper prescribers.
When you are faced with a patient who thinks they have become suicidal on treatment – the first scientific task is to work out what is happening. This is a judicial task. Key to this is the conversation with the patient who may say ‘Doc I’ve been depressed and suicidal before but this was different – I think it’s the drug – it cleared when I lowered the dose’.
This engagement is a scientific engagement with the data – the person. If you conclude the drug has made the person suicidal but the published academic adverts do not seem to support this, the next scientific task is to reconcile the mismatch.
In the case of SSRIs and suicide, you find:
- companies breached FDA regulations in hiding events
- companies misapplied statistical methods
- the entire literature on these drugs is ghostwritten
- there is no access to the people in these trials for independent scrutiny
- FDA don’t have and have never seen the data
When you get to the bottom of this you find what your patient has told you squares with the real science behind the apparent science. Case reports offer the only science in clinical psychopharmacology.
Slide 19
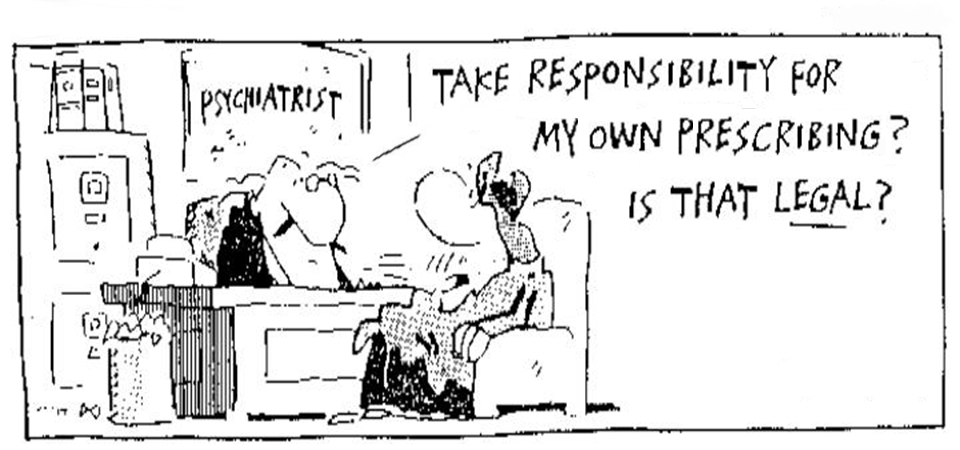
We in psychiatry used to be great at telling people to Take Responsibility for your Own Life

Slide 20
The challenge for us now is to Take Responsibility for our Prescribing
Slide 21
The quote is from Louis Lasagna the man responsible for incorporating RCTs into the 1962 Food and Drugs Act, who soon after came to doubt the wisdom of what he had done.
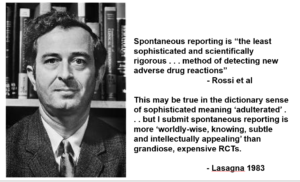
This is a clever use of the word sophistication – which I doubt if many non-native English speakers will immediately appreciate.
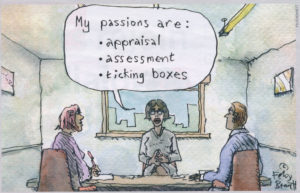
If you smile at the poor medical candidate here whose passions are not about saving patients from the effects of poisons, engaging with them in some of he most important conversations possible but are instead appraisal, assessment and ticking boxes – you shouldn’t.
You know the interviewers are equally constrained to ask exactly the same questions of each candidate and not be remotely intuitive. You go along with this and the College supports this totally – on the advice of management consultants.
Slide 22
The judgement calls of clinicians are now a problem. They are pitched against RCTs, which supposedly deliver valid knowledge. Even if done by angels RCTs don’t evaluate drugs.
Another problem for the generalist featured here is the increasing size and crazy nature of drug cocktails that partialists – like us – recommend.
As a family doctor recently said to me – if I refer a patient to a cardiologist the response will often be there is no cardiac issue. Ditto for gastroenterological or respiratory referrals. But a psychiatrist will never respond this patient is normal.
Life expectancy is now falling as a result – and was before Covid. Polypharmacy is almost certainly one cause – and it has become harder to establish if a drug is causing a problem, not because of lack of access to trial data or the ghostwriting of the clinical trial literature but because people are on so many drugs that picking out the causative factor has become harder. Medicine as we have known it for two centuries is over.
Slide 23
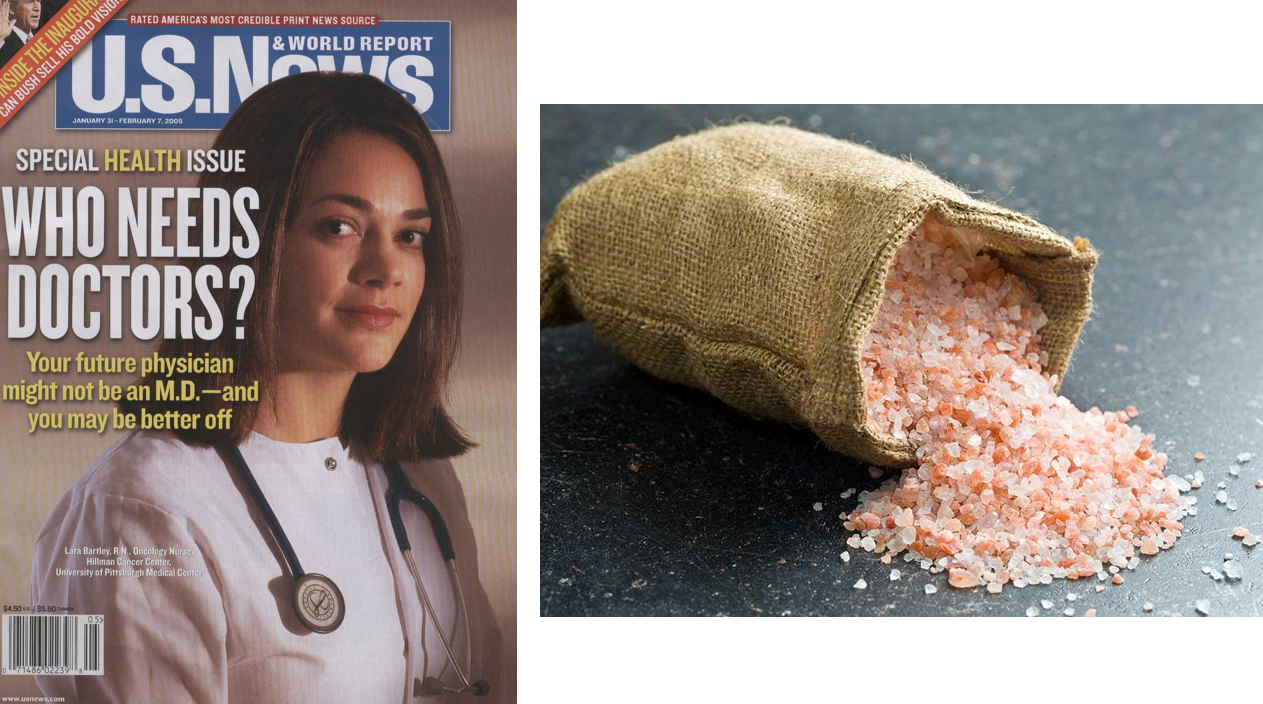
In 2002, a New Labour plan for the National Health Service foresaw nurses replacing doctors for many tasks that can be standardized from colonoscopy to prescribing.
This advert in a US magazine from 2004 envisages the same future.
We are now training Low Salt Doctors and have no room for old style clinicians who listened to and saw patients. The people on the coalface will be nursing staff and pharmacists, who will keep to guidelines. If doctors have a role it will be as managers enforcing processes – I should say bureaucrats enforcing processes – managing the risks clinicians and patients might pose to the organization.
There will be no option for many patients unable to get treatment for harms but to resort to being entrepreneurial.
We now work in health services not healthcare. Our work is managed on the basis of metrics and criteria – things that make psychiatrists look like doctors and manageable – things that empty out the concept of a professional.
Slide 24
Schizophrenia used to be our core business. It is vanishing.
This may not be a problem if we have all become American and the business of both the professions and pharmaceutical companies is growing business rather than eliminating it.
Psychiatry has been rather successful at growing business – perhaps even more so than other branches of medicine and even more so since its turn to the body and drugs that can be impossible to stop.
The main growth area now centres on antidepressants and minors.
All 15 pre 1990 RCTs of antidepressants and depressed minors were negative. All 30 post 1990 RCTs Negative. This includes the two Prozac for children trials that got it licensed – along of course with the 3 negative paroxetine trials that FDA agreed with GSK’s view that they were negative but were still willing to approve paroxetine for minors and not mention in the label that the trials were negative.
Psychiatry has the proud honor of hosting the greatest known divide in medicine between what the trial data shows when accessed and the claims in the peer reviewed academic literature.
Despite 45 out of 45 Antidepressant trials for depression in minors being negative, these are now the second most commonly taken meds by teenage girls.
Greta Thunberg’s generation are out protesting about the chemicals in the environment but swallowing more chemicals than any other generation ever did.
If you stand up to the management, regulatory, political and other tanks, these kids will trample you to death in an effort to get at the eucharist they see as their due.
****
See The Nature and Meaning of Psychiatry
Peter Selley sent the image below with a comment – RSM attendee had lucky break
Gunfight at the O.K. Corral …
In Topical Parlance, “Cold Gun” “Hot Gun”, a shot is fired from a gun that is not a blank –
It used to be said a lot that Doctors were playing “Russian Roulette” with patients’ lives when prescribing antidepressants like Paroxetine with little or no discussions about adverse events or how to safely come off them. In most instances where serious problems started happening, the Doctor would not believe what he was hearing and from this a whole ‘Harmed Community’ has developed.
It would be OK if the drugs were ‘blanks’, but they are not and it seems utterly ruthless for any psychiatrist to deny how dangerous psychotropic drugs can be.
The ANTLER Study
Prof Sir Simon Wessely, Regius Chair of Psychiatry, King’s College London, said:
“This is a very important study. It mirrors one of the first randomised controlled trials ever undertaken in depression, which found some benefit to staying on antidepressants for at least six months after you had recovered from a depressive illness. Now we know this applies for an even longer period. On the other hand, the other good news is that if you do want to come off antidepressants for whatever reason, this can also be done safely over a couple of months. So now patients taking long term antidepressants can make an even more informed choice than before. Yes you can come off medication, provided it’s done slowly, but there is an small but not insignificant risk of another illness. As ever there is no right answer, but this study provides more information to assist people in making up their minds.”
This is death-defying nonsense. He has been playing with his ‘Holster’ for far too long.
He has spoken quite clearly that he finds antidepressants ‘safe and effective’.
To then come on and to ‘assist people in making up their minds’ is a crash-course.
‘safely over a couple of months’ is disingenuous baloney.
Wendy Burn and her letter to The Times was a ‘real-gun’ moment.
Wendy Dolin flew thousands of miles to give a presentation about Akathisia and how this condition led to the death of Stewart Dolin.
She couldn’t even bring herself to acknowledge Wendy in the RCP Stopping Antidepressants.
Louis Appleby and his view on Akathisia to Dee Doherty.
A real smoking-gun.
In the Real-World-Corral these ‘antler-antics’ are terrifying and another terrific lecture comes our way, casually thrown away in end of lecture comments –
“Cold Gun” “Hot Gun” …
Professor Glyn Lewis
HC Deb 27 July 1998 vol 317 cc38-9W38W
§Mr. Hancock
To ask the Secretary of State for Defence, pursuant to his answer of 29 June 1998,Official Report, column 7, if he will make a statement on the medical career and research background of Professor Glyn Lewis. [52064]
https://api.parliament.uk/historic-hansard/written-answers/1998/jul/27/professor-glyn-lewis
Most common antidepressant barely helps improve depression symptoms, ‘shocking’ trial finds
https://news-media.top/most-common-antidepressant-barely-helps-improve-depression-symptoms-shocking-trial-finds/
Professor Glyn Lewis, who led the research at University College London, said: “We were shocked and surprised when we did our analysis.
“There is absolutely no doubt this is an unexpected result.’
“Our primary hypothesis was that it would affect those depressive symptoms at six weeks and we didn’t find that.
“We definitely need better treatments for depression, and we need more research in this area.”
He suggested that new, more effective classes of antidepressants could be based on ketamine, psilocybin, the psychedelic in magic mushrooms, and anti-inflammatories.
It is thought that roughly four million people in England are long-term users of antidepressants.
Prescribing data shows that SSRI’s such as sertraline make up 54 per cent of antidepressant prescriptions.
Scientists have responded to the new study by pointing out that some of the patients had very mild symptoms of depression to start with, making it less likely that sertraline would cause an improvement.
However, others have pointed out that this is exactly the basis upon which GPs tend to hand out the drugs in practice.
Dr Gemma Lewis, who co-authored the new research, said: “I think it’s really important to understand that anxiety symptoms are very, very common among people with depression.”
She added: “It appears that people taking the drug are feeling less anxious, so they feel better overall, even if their depressive symptoms were less affected.
“We hope that we have cast new light on how antidepressants work, as they may be primarily affecting anxiety symptoms such as nervousness, worry and tension, and taking longer to affect depressive symptoms.”
Professor Helen Stokes-Lampard, Chair of the Royal College of GPs, said: “It is well-established that it often takes a while for patients to feel the full benefits of modern antidepressants and that they work best when taken for significant periods of time, which is one reason why doctors will often review patients after several weeks of use and then prescribe a fairly long course of the drugs, if they appear to be beneficial.”
A randomised controlled trial assessing the use of citalopram, sertraline, fluoxetine and mirtazapine in preventing relapse in primary care patients who are taking long-term maintenance antidepressants (ANTLER: ANTidepressants to prevent reLapse in dEpRession): study protocol for a randomised controlled trial
Larisa Duffy, Faye Bacon, Caroline S. Clarke, Yvonne Donkor, Nick Freemantle,Simon Gilbody, Rachael Hunter, Tony Kendrick, David Kessler, Michael King, Paul Lanham,Gemma Lewis,
Dee Mangin,Louise Marston, Michael Moore, Irwin Nazareth, Nicola Wiles & Glyn Lewis
https://trialsjournal.biomedcentral.com/articles/10.1186/s13063-019-3390-8#:~:text=%20Methods%2Fdesign%20%201%20Study%20design.%20The%20ANTLER,method%20of%20recruitment%20will%20answer%20a…%20More%20
experts
86 on
https://www.casemine.com/judgement/uk/5a8ff7d860d03e7f57eb26dc
The Back Stories…
Going Ga Ga – See a GP specialising in Medications … swivelling a narrative
An epidemic of anxiety among the over-60s is unearthed after Dr Ellie Cannon revealed her own 15-year mental health struggle
By EVE SIMMONS FOR THE MAIL ON SUNDAY
PUBLISHED: 22:00, 30 October 2021 | UPDATED: 22:03, 30 October 2021
https://www.dailymail.co.uk/health/article-10147565/Dr-Ellie-Cannons-mental-health-confession-unearthed-epidemic-anxiety-60s.html
The article has unleashed a hidden tide of anxiety disorders among older adults.
‘Anxiety is a very common problem we see in older patients. Medication to treat anxiety and depression is among the most common I prescribe,’ says Dr Clare Gerarda, a GP specialising in psychiatry.
‘As you get older, you’re more likely to suffer serious health conditions and the stress of physical illness often triggers mental health problems.
If It’s Not ‘One’ It’s The ‘Other’…
“Unearthing” probable calamitous prescribing to the elderly – just gaga…
I watched “The Standardization of Psychiatry” on Youtube and tried to leave a comment.
It was deleted though I tried Several times.
So I left it on my blog ( https://hellaheaven-ana.blogspot.com/2021/10/my-comment-on-youtube-was-deleted-it-is.html ) and now here:
“Thank you Dr. Healy.
You always give the broad picture of everything. Never heard of a physician that put the political, economical and cultural aspect of what they are explaining.
“So tiny and…” my conclusion is always the opposite: “So tiny and causing so many illness.”
I beg your pardon? 20:37 “… market Zoloft neither the names in the authorship line nor the people who run the trial, nor the ghostwriters, nor the FDA or the MHRA will have seen the data from these trials.”
“So I´ve written to NICE, and, MHRA, and EMA, and FDA, all the major journals, all the politicians, the minister of health in all the departments of health in the western European archipelago, – that’s England and Ireland for those who weren’t sure what it is, – and they all agree that the literature was ghost written and there’s no access to the clinical trial data. Their response is to take the escape route that I offered them which is that it’s not our job to police the medical literature raising the question of whose job is this.”
Stop the world, the planet… the universe.
I’m glad I still have some innocence left and indignation.
Funny that UK Parliament talk about ghost writers in their 2005 review “The Influence of Pharmaceutical Industry”.
Suicide ideation not related to the depression but as a side effect is also there.
https://publications.parliament.uk/pa/cm200405/cmselect/cmhealth/42/42.pdf “
Just an aside about schizophrenia being on the decline, and why psychiatrists are not curious about the causes. To listen to leading psychiatrists in the USA, you would think schizophrenia was 1) at least as common as ever, if not more so, and 2) totally treatable thanks to amazing advances in Brain Science – but only if Caught Early!
I suspect the flood of new “anti-psychotic” medications has led to a real dumbing-down of the whole medical profession, shrinks especially. They no longer realize what a wide variety of factors might cause a person to hear voices, develop “paranoid” fears or otherwise loosen their grip on reality for a time. No, it is all “psychosis,” which is conflated with “schizophrenia,” so that every patient is assumed to have a primary Brain Disease. A lot of this seems like “reasoning from pill to illness.” If I’m giving Anti-Psychotics to treat this illness, then it must be a Psychotic Illness, right?
This is not a new problem – in fact one of the purposes of the DSM-III was supposed to be fixing such diagnostic sloppiness. Especially the American tendency to label any serious mental-emotional problem as Schizophrenia. Freudians and other “psychodynamic” shrinks had a very bad case of this disorder, and “biological psychiatry” was supposed to cure it by making definitions more scientific. Oh well.
The new phase of the disorder is an obsession with psychotic or even “pre-psychotic” symptoms in teens and young adults, or what is labeled First Episode Psychosis. The very name assumes the person’s current crisis is the “first episode” of a lifelong illness, which should be arrested or at least managed with long-acting injectable antipsychotics. As near as I can tell, most of the money in psychiatry is flowing into these very lucrative injections, which can force “medication compliance” for up to a year at a time. That poses a risk of turning “lifelong illness” into a self-fulfilling prophecy.
How to insult a GP -or maybe some would like even more decision making removed .
Pulse Today
A major London hospital trust has launched a trial requiring GPs to use advice and guidance (A&G) services before referring patients.
The trial currently spans 13 specialities but if successful, the measure ‘could become the default’ for all services across the trust.
Barts Health NHS Trust announced last week that ‘from this month, GPs wishing to refer a patient into some Barts Health services will first need to consult with hospital specialists’ via A&G.
It said: ‘The change is being trialled across 13 specialities and could become the default for all of our services.’
A Barts spokesperson told Pulse that GPs will no longer be able to make ‘direct referrals’ to these specialities and that A&G will become the ‘single point of access’ to the service.
GPs will have to request the A&G function on the e-referral service (eRS) used by the trust and the request will be converted into a referral ‘where appropriate’, they added.
They will receive a reply from the hospital specialist ‘within five days’, either with advice on how to manage the patient themselves or informing them that the hospital will organise an appointment, the trust said.
Re Spruce’s comment flagging up Daily Mail artice – have sent the video of DH lecture to the authors of the article
e mail london@rochealthservices.com
Why is it that when I take my B12 shot it hardly hurts at all, but when I take my Abilify shot it is sore for at least a day or two? My suspicion is that my body likes the B12 a lot more than the Abilify.
Among many reasons to be disturbed about taking psychotropics, this is one of the worst. https://pubmed.ncbi.nlm.nih.gov/18626887/
It appears to be published around 2008, Has anyone made any progress in this field of research? From what I can tell so far, (and what I vastly suspect) this only scratches the surface of the biological effects of Psychotropics. Patients need to be aware of what kind of supplements to take to counteract the adverse biological effects of psychotropics. They also need to be aware that science is still learning about what these drugs really do and that there may be unknown unintended consequences to taking them.
If psychiatry is to ever resurrect itself in a popular way as a moral practice, it should take a much stronger role in educating the pro and con realities of psychiatric drugs to the patient and the public. Informed consent should be one of the corner stones in a doctor patient relationship within Psychiatry. If Psychiatry does not strongly adopt open and transparent informed consent very soon, It may continue to have ungodly amounts of power over some of the most vulnerable in society but it will likely flush its respectability as a real medical and scientific enterprise down the toilet in cut time.
Many of us who are on the short end of the societal stick and who feel (rightly so) stuck in the system, clearly see the rotten termite infested side of mental “health”. We feel the insane effects of the drugs and we see the stubborn desire of those who prescribe to not look for or even consider alternative treatments.
We are told over and over again the false narrative about our “chemical imbalance”. (often by hospital staff who are greatly pressured to deceive the patient because their job depends on pushing what is prescribed) The truth about the DSM is generally hidden especially in the hospital as is any inconvenient truth about psychiatry. If people are being deceived or coerced so that they adhere to possible life saving and necisary psychotropic treatment, (weather it is life saving or necisary comes down to a debate I am not informed enough to take on like someone like Robert Whitaker would) that means in the case of mental health, sometimes (or actually quite often) the ends justify the means. Rarely does this not become unethical or immoral. At best it is a very dangerous slippery slope. At worst, well, who really wants to take that risk? (obviously mental health but one has to wonder, who really has the mental illness here?)
Often those of us stuck in the system naturally despair over endless dirty treatments for our “incurable” disability (often created or exacerbated by the drugs). We then are offered more “medication” for our “depression”. When we are doing fine we are instructed to stay on our meds, when we are not fine we are given more meds. When we try to explain this Chinese handcuff downward spiral, no one seems to give a flying (well) thought about it. Everyone around us with any power seems to adamantly want to obey and get direct instruction from the Psychiatrist or any medical “expert” on our care. The psychiatrists however tend to heavily rely on social and economic pressure to make their judgement, knowing full well (but not often admitting) that their decisions (some easier than others) are really a highly educated guesses.
No one knows or has an example of a truly healthy brain (not even the Psychiatrist, believe me, I asked). So really, general Psychiatry is just a very dangerous pharmacological (often poly-pharmacological) wack-a-mole guessing game to any symptom that appears to be undesirable or perceived as dangerous. The result being an explosion of docile or angry unemployed institutionalized chemically sterilized (or in many cases sexually excited) and often chemically lobotomized highly medicated individuals with a plethora of neurological and biological problems. Psychiatrists know this is a problem, but they are continuously swept up in the social and economic currents that keep the machine going. They need to develop a moral backbone. Really, they need to have a heart which can be hard to instill in a big Pharma influenced academic environment. Doing so also very well could mean a slimmer wallet, and there lies the rub for many in the industry.
I do however see some hope. Much of the younger generation, as usual in any society, is very counter cultural. Which means more consideration for alternative medicine. I also see big Pharma becoming more desperate and possibly more dangerous for social and economic reasons, which would create a societal backlash. I see more of a revolving door between idealistic psychiatrists and economically driven Psychiatrists as some old Psychiatrists wake up and some new blood comes in for the promise of big paychecks.
I see websites like Mad in America continuing and likely growing in an underground fashion, and I see the obsession with the established poisonous medical industry dying a very hard death. (probably not unlike the kind of death many chronic psych patients face) I see more research in the promising field of how the microbiome affects biology and mental health. I believe individualized medicine is coming with a balanced approach with what is now considered conventional medicine in the most extreme cases, but the bread and butter in what we now call alternative medicine most often for preventative purposes. I see the current technology of pharmaceuticals being treated soon one day much the same way we treat artificial sweeteners. I predict that a growing body of evidence will show that nearly all current mainstream psychotropic pills are dangerous to your microbiome and ultimately to ones body and that LAI’s as we know them today are overall toxic to human biology.
I don’t quite know where psychiatry will go. There seems to be some promise in patented microbiological living or somewhat living organisms like viruses, bacteria and fungi. The old rift between psychiatrists and chiropractors may completely disappear if psychiatry starts looking at the benefits of natural supplements. Maybe psychiatry will go back to its roots of psychoanalysis or psychotherapy. Maybe new drugs will come out that are not so neurotoxic. The big question I have is, can big Pharma ever improve on mother nature, or really can anyone? I guess that comes down to the evolution intelligent design debate which for me gets pretty complicated.
“neither the names in the authorship line nor the people who run the trial, nor the ghostwriters, nor the FDA or the MHRA will have seen the data from these trials.”
And more….
https://twitter.com/WhatsUp_Canada/status/1454172354905448449
Good to read something that takes common sense into account.
I clearly remember taking one Prozac pill and feeling actively suicidal; Effexor caused me to be ever so calm (and thrilled to be) for maybe an hour, then the flip side with extreme agitation; Remeron, Zoloft, Paxil, and others each had a very different effect. It was all like going to IKEA, a extended difficult experience but a few absolute helpful people and treasures along the way.
I.m tossing up whether to rummage through their tool box as The GMC is notorious for taking
months which they can drag into years using various ploys on past experience of working as an advocate, to deal with the predictable runaround
Your GMC enquiry (The Call centre handler -sorry ‘Contact Centre Advisor ‘might have spelt my name correctly by the way – ) But worth having another concern on the GMC records along with a previous complaint by a group concerned about her.
gmc@gmc-uk.org
11:24 AM (1 hour ago)
to me
Dear Suzanne
Thank you for your email about your concerns.
If you have serious concerns about a doctor, you should raise them with us via our concerns tool which you will find in the concerns section of our website.
These concerns could include:
serious or repeated mistakes in patient care
failure to respond reasonably to patient needs (including referring for further investigations where necessary)
violence, sexual assault or indecency
fraud or dishonesty
a serious criminal offence
abuse of professional position, eg an improper sexual relationship with a patient
discrimination against patients, colleagues and others
Please be advised that you will also need the doctor’s full name and GMC number in order to submit your concern to us.
If you would like to discuss this further, please call us using the number below or reply to this email.
Yours sincerely
Claire
Claire Hall
Contact Centre Adviser,
Registration and Revalidation Directorate
Telephone: 0161 923 6602 (+44 161 923 6602 from outside the UK)
Website: http://www.gmc-uk.org
Re . Dr Ellie Cannon
29 August 2019
‘In an era of fake news, TV doctor Dr Ellie Cannon is the much-needed antidote to health myths.
She is also a blogger for Pulse and has tackled issues including the anti-vax movement and fighting cervical cancer.’
Decided to go ahead with complaint to the GMC re misinformation propagated by Ellie Cannon GP re ADs
plus lack of response fro the sugery manager – there is an obligation to respond CCG is trying again
Hello All (to madintheuk)
just a bit of an update – Ellie and the surgery manager have an obligation to reply.
Complaint has been forwarded to GMC – will take ages but will keep you informed
All the best – take care
susanne
———- Forwarded message ———
From: COMPLAINTS (NHS NORTH CENTRAL LONDON CCG)
Date: Wed, Nov 10, 2021 at 5:08 PM
Complaint regarding the seriously misleading information broadcast by Ellie Cannon
Cc: COMPLAINTS (NHS NORTH CENTRAL LONDON CCG)
Dear (susanne)
Thank you for your response.
GPs are not employed by Clinical Commissioning Groups for their general practice work, and we are also not directly responsible for the performance management of GPs. We are co-commissioners with NHS England. We will forward on your complaint to ITV and make sure you are copied in. ITV is responsible for the information that they broadcast on their programmes, and for ensuring that a balanced perspective is presented, so we feel that they would be best placed to respond.
In regards to the complaint you have made about the practice’s contact information, our primary care team will follow this up with the practice to ensure it is addressed.
Best wishes
Brett
Brett Vallance
PALS, Complaints & FOI Manager
North Central London CCG