On Wednesday February 10, I gave a lecture at the Therapeutics Initiative (the T.I.) in Vancouver about the Permanent Sexual Dysfunctions SSRIs and other drugs can cause. See Sex and Evidence Based Medicine.
The damage done by these drugs often extends beyond a total and complete inability to feel sexual desire and pleasure to a total inability to feel pleasure of any sort and a profound loss of identity – a living death.
These Enduring Sexual Dysfunctions affect black, brown, yellow, and white. They affect rich and poor. Women and men. Young and old. No group on earth is spared – although at the moment white people are bearing the brunt of this plague.
The February lecture makes clear that, while the conspiracy theories some white people have that they are being replaced are crazy, the enduring sexual dysfunctions are bringing about just this in reality.
White people are replacing themselves because so many of them are taking these drugs that close to 1 in 5 of them can no longer make love or when they do if they get pregnant the drugs double the rates of miscarriage, and double the rates at which any children born will be autistic, hyperactive, debilitatingly anxious from a young age or have serious cardiac or other physical defects.
White people are in the firing line because of their collective and individual belief in the promise of technical progress. Black people are still more likely to turn to their people, a community, for support, and Muslims turn to the Ummah, which means roughly what The Invisible Body used to mean for Catholics. No Protestants and probably few Christians of any sort under the age of 40 have any sense of what an Invisible Body might be.
I’m not bothered by White people being replaced. I am bothered by the people with enduring sexual dysfunctions who are in touch with me who kill themselves or seek Medical Assistance in Dying for this or the related Treatment Resistant Depression.
The February lecture has introduced a censorship into the T.I. because 2 of the 300 people in attendance objected to one slide featuring the Real President of the United States. The version of the lecture now on the T.I. site no longer features the original slide (number 10). For weeks until a compromise was reached, T.I were happy to cut the slide and with it the chunk of lecture that went with it without which the lecture doesn’t make sense – this was one of the two ventricles that kept the heart of this talk beating.
They are now planning to join the pharmaceutical industry in screening everybody’s slides before they give a talk.
A slide that once would probably have given Donald fond memories – available on Sex and Evidence Based Medicine. – caused more concern than the serial and increasing deaths of young people who die because of their accurate perception that no-one gives a fuck and the system is going to do nothing to try and solve the problem. Die because they get laughed at by doctors, and other healthcare staff.
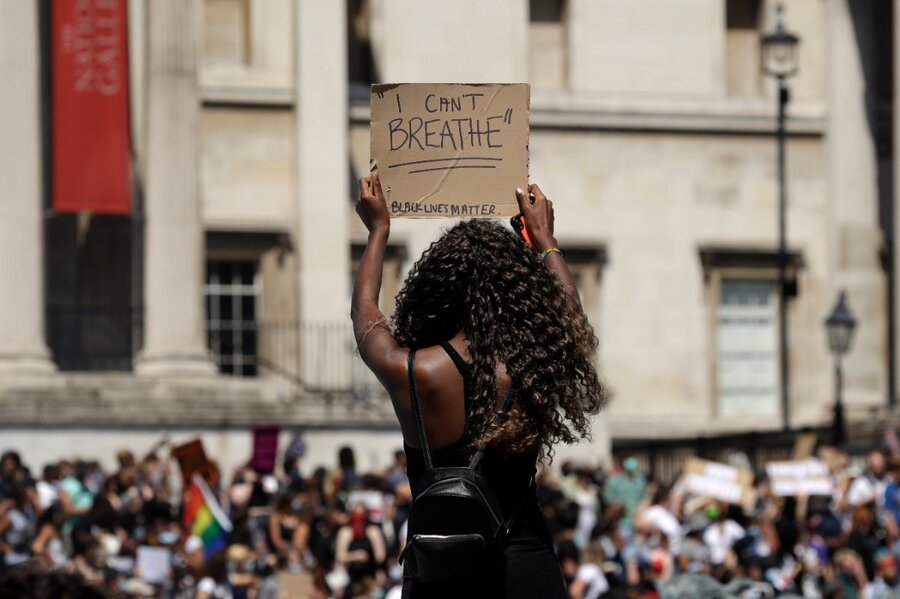
I can’t breathe
On Wednesday February 10, as I gave this lecture, Janet, a mother in America, working in a senior healthcare post, found herself unable to breathe. She had been emailing me regularly for over a year saying this day would come. She emailed me when she caught a breath.
I can’t breathe my baby is gone due to medicine that was supposed to help him. He is in God’s arms but I want him here.
Her 20 year old son, Jordan, who had Post-SSRI Sexual Dysfunction (PSSD) had taken his own life as she had known for over a year he would.
If it was my son, I’d imagine I’d have homicidal thoughts, like many black people have after encounters with the police, Being Black, and I can imagine it might be difficult for me not to act on them.
Medical Kidnap
S, a young woman, somehow plucked up the courage to come to me some years ago, trusting her parents who both worked in healthcare.
She had been shy and anxious starting a new job and mentioned this to a family doctor who showed more wisdom than most and reassured her that he would support her. But on another visit to the clinic a different doctor supported her in a different way – giving her an SSRI.
She disintegrated rapidly, ending up in hospital, diagnosed as schizophrenic and given a cocktail of drugs every one of which made her worse. Her father, a doctor, was powerless to help. He rapidly became viewed by the system as part of the problem rather than the solution which he sensed lay in the opposite direction to what the system seemed hellbent on pursuing.
There are nearly 30 posts under the Medical Kidnap heading on the RxISK blog all powerful and some of the earliest ones in particular featuring Teresa Pocock and S in Kidnapped Daughter, Kidnapped Daughter 2 are chilling.
Her parents finally got S back. Badly damaged. They figured they had no option but to take her out of the country and finally to bring her to see me.
She has remained drug free ever since and has slowly recovered from a lot of physical damage and even more damage to her confidence.
Years later, she remains as unwilling to see any doctor for anything as Barack Obama in shabby clothes, or Joe Biden if he were black, or any real black man would be to walk into a police station and mention they were having homicidal thoughts after being jumped on by some policemen a few weeks before – see Being Black.
She is just one of many people I know in a similar situation – people who might make a bad mistake in response to an invitation to come along and see one of our doctors, and say ‘I’d sooner die than go to see Dr X’. Its not safe dealing with health systems these days. Most people don’t know this. A growing number have learnt the hard way.
Discarded by GSK
Last week, RxISK told Shane Cooke’s shocking story in Discarded by GSK. Here was a young man driven into a delirious state by a drug. It should have been clear to those treating him the drug was causing his problem.
An idiot of a judge jailed him for two years when he had done relatively minor damage to the property of a service who said they would help him, but made everything worse at every step, and in the end refused to help at all despite every wall of its buildings being festooned with slogans like We Help because We Care.
Shane’s case echoes that of the Guildford Four – four innocent Irish people jailed by a corrupt English police and legal system that wanted to be seen to have caught and incarcerated people no matter – any Irish fucker would do.

Gerry Conlon, one of the four, the hero of the movie In the Name of the Father never recovered even after they won their freedom 15 years later despite the very heights of the British legal system making it clear that they should stay in prison, even if innocent, in order that the public doesn’t lose confidence in the police.
Shane was imprisoned in order that the public doesn’t lose confidence in its drugs.
Most Irish people know where they were when the Guildford Four were released just as most Black people (and lots of others) know where they were when Barack Obama came out on a Chicago stage as President Elect. But Irish people, as my Black arm-wrestler made clear to me (Being Black) have never had to put up with anything like what Black people have to put up with.
The one moment my arm wrestler showed some discomfort was when I mentioned that the horrors the Irish have been through haven’t made us nice people – we are among the most bigoted, and racist people on earth in my opinion. He couldn’t accept that this might be true for Black people also – even some of them.
In my opinion Black people in general are a lot more decent than white people but being oppressed does nothing good for the soul. Being an oppressor does nothing good for the soul either.
Shane’s life was destroyed by prescription drugs. If I were him I’d have been very inclined to give the system a legitimate reason to jail me. But what Shane is now doing shows that somehow some of us rise above unimaginable setbacks and get to a point of doing things to help others.
Black, or Indian, or Part of the System?

Some will never get a chance to give back – see The Man who Thinks he is a Monster.
James Holmes was put on Zoloft for shyness by a University shrink, who cranked the dose up as he tried to intimate that things were going badly wrong. She told him anything that happened was his responsibility.
What happened was 12 people died and 70 were badly injured at a premiere of Dark Knight Rises in Aurora Colorado in 2012.
Holmes was innocent (in my opinion – having spent time with him). But he is now serving the third longest sentence in US history because his public defenders felt they couldn’t persuade a jury that the entire literature on which all doctors depend is a Fake Literature, ghost written, sometimes claiming a drug works well and is entirely safe when FDA know the trial data is negative and points to serious problems but they say nothing.
How do you take a jury to a point like this. In New South Wales in 2001, a prosecutor (like Kamala Harris once was) told the judge it was obvious this man, David Hawkins, didn’t kill his wife. The Zoloft he was on was responsible. Hawkins walked free.
My Black man and every one else featured in this post and me and many of the rest of us figure we have to stick to due process – take our grievance to the law rather than take the law into our own hands. Pretty well no-one knows that when it comes to the effects of drugs the legal system is entirely corrupted and will jail us rather than let people lose confidence in their drugs.
Rather than let a jury and the media hear that the entire literature on these drugs is ghostwritten etc, prosecutors like Kamala Harris do a deal with the defence to lock someone away till after the earth has burnt to a cinder in exchange for not-executing them – even when someone like James Holmes would have preferred to be executed.
The families and friends of everyone killed or injured in Aurora are being denied the truth of what led to these deaths and injuries.
Kamala – are you Black or Indian or part of the System? What about you Alexandria?
Brenda Hale, a.k.a Spiderwoman, until recently the Chair of the UK Supreme Court was viewed as the bravest women in Britain in 2019 when she faced down the government. But when it comes to the Holmes, Cooke and O’Neill issues which call into question the capacity of the justice system to do what it is supposed to do without fear or favour, Brenda is a System woman – see The Perfect Killing Machine and There is no Sanity Claus.
Shipwrecked Heroines
There are many heroines, and a few heroes, in Shipwreck of the Singular. Right up there at the top of the list is Anne-Marie Kelly. (This post might have worked well for International Woman’s Day except that tokenism is exactly what these issues do not need).
Put on an SSRI she became alcoholic, lost her job and ended up with a criminal record and jail sentence for annoying the police. She figured the Paxil she was on was causing the problem but got laughed at by her doctor and then by Alcoholics Anonymous, who told her that her thinking proved she was an alcoholic.
As things fell apart, without any background in healthcare, and even though an early school drop-out, she began researching SSRIs and worked out exactly what was happening and how to put it right – teaching me things about the Serotonin system in which I have a PhD.
Leaving me figuring that Motivation counts for more than Expertise.
She too was jailed by a miserable magistrate and had her appeal to have her criminal record overturned by an equally miserable and self-righteous judge who paid no heed to the fact that while almost no-one else agreed with her, the pharmaceutical industry did agree and were developing drugs based on her ideas as her expert report pointed out. The failure of her Appeal made it impossible to get a job.
Reflecting on an unbelievable nightmare, kept going perhaps to some extent by the fact that telling her story has saved hundreds of others, helping them to pull themselves out of a downward spiral into chaos and disaster, her view is
‘I think we are all here to learn about the difference between love and hate. Our existence is to teach love to one another‘.
Shipwreck takes on the issues in Being Black and makes the claim that whether we are Black or White, Female or Male, Old or Young, Rich or Poor, the most profound divide between us is the divide between the Fortunate and the Unfortunate.
Not even losers like the company of losers. The ultimate losers in our society are the Drug Wrecked. They have had acid thrown in their face. They need to find an Ummah, a People, an Invisible Body.
Even more than those afflicted with AIDS in the 1980s and 1990s, the pioneers in doing this have been the Indian women disfigured by acid thrown in their faces who have found each other and provide a support they can get from nowhere else.
This world desperately needs heroism like this, leadership like this – from the bottom up – rather than looking to experts or those who claim to represent ‘us’ but increasingly make vassals of us.
Seeing a documentary featuring James Holmes was the reason I contacted David and got involved with the blogs.
People put into yet another insultng category of human being whether they agree or not ,BAME, are still not in a position to translate their anger and hurt into changing the systems which excercise power over our lives. Their mistrust of the medical/political is right now being challenged by policies of paying the winners in their own communities , although they don;t actually live in these ‘deprived’ areas, to go phoning and knocking on doors for a few quid a time,to persuade vaccine refusniks, mainly poor, disempowered groups , to get vaccinated. With claimed %70 sucess. They will likely need doctors- it’s hard to refuse. These are state sanctioned blackmailers. who feel they have become part of the ‘elite’ by doing their bidding. So Softly softly spreading fear. I am declining, yesterday ‘my’ optician asked if I had been vaccinated – I was nervous about saying no. Likewise a neighbour who previously hadn’t spoken for a year gave a ‘look’ to the ‘no’. How soon will pharma and the medical profession have driven a wedge through yet another area of society they are so concerned to control. Yes it’s about pharma and their filthy lack of morals , the love of unaccountable power by their networks shames them . People in parts of the world are being brutalised by those who have been brutalised themselves just like in Ireland It is horrendously exhausting to keep challenging the system – during the worst effects of harmful drugs, almost but not quite impossible. Shaking off the the shackles of drug induced acceptance of being brutalised is a triumph of shared humanity which still exists whatever the colour of our skin. I am not sure I could love those who harmed me at my most vulnerable even if I understand the reasons to some extent – their ideal of a successful life is to live a corrupted life and we only have that one to decide to live decently -that’s if we survive being pushed to the brink with enough energy left to take action however small, however unrecognised. Suicide and homicide are one way out of it , lambs to the slaughter mainly, Just like those being shot at the baricades .But there is one worry which bugs me -that pharma and their networks such as the college of psychs could turn this potential for suicide and homicide as an effect of drugs ,which is becoming more public, into yet another deliberate way of creating fear of people with especially more severe mental health problems. What then – genetic modification -Neuropsychiatry -Greater involuntary levels of control to mess with us.
“Her exile from mainstream humanity” – Dr. Doctor – Kidnapped Daughter
Christopher Lane Ph.D.
How Schizophrenia Became a Black Disease: An Interview With Jonathan Metzl
In the late 1960s, schizophrenia’s profile as a disease changed dramatically.
Posted May 05, 2010
https://www.psychologytoday.com/us/blog/side-effects/201005/how-schizophrenia-became-black-disease-interview-jonathan-metzl
I also document in the book how associations between insanity and the civil rights movement played out extensively in American popular culture, and helped to shape the emergence of a much wider set of stigmatizations of schizophrenia—that it was an unduly hostile or violent disorder. I look closely at changing twentieth-century American assumptions about the race and temperament of schizophrenia through sources including American medical journals, newspapers, popular magazines, historically Black newspapers, studies of popular opinion, music lyrics, films, and civil-rights memoirs. I also reproduce unbelievable pharmaceutical advertisements that show angry black men protesting in the streets as ways of selling antipsychotic drugs.
But today you also see increasing numbers of scholars like myself who believe in the therapeutic and even potentially liberatory promise of the profession, while remaining deeply concerned about such issues as the impact of the pharmaceutical industry, the stigma surrounding diagnosis, and the expanded use of psychotropic medications, to name but a few.
“only during the civil-rights era did emerging scientific understandings of schizophrenia become enmeshed in a set of historical currents that marked particular bodies, and particular psyches, as crazy in particular ways. The tensions of that era then changed the associations that many Americans made about persons with schizophrenia. Ultimately, recent American racial history altered more than the meaning of mental illness: it changed the meaning of mental health as well.”
Paul John Scott @pauljohnscott
Juror being evaluated in Chauvin trial now correctly used the word “killed” in connection to the death of George Floyd — it was the determination of the ME — and defense is treating it as an opinion. Why is this allowed?
Doctors make exiles out of the drug wrecked
What is unfortunate is each doctor who has a suicide on their books is not fully investigated for crimes against humanity as in the real world they don’t have a leg to stand on and any doctor having their knee on your neck is culpable none more so if he has “killed” his patient and/or deliberately ‘under cover’ has caused severe distress and possibly incarceration.
Double-standards and double-dealing…
‘Don’t be frightened – they’re here to help you’ ….the horror of the mental health system – suicide; homicide and lets not forget murder by any other name
Published18 February
Protesters gathered in Newport following Moyied Bashir’s death
More than 100 protesters have gathered in Newport following the death of a man shortly after police were at his house.
The IOPC said Mr Bashir’s condition worsened after police officers arrived. He was taken to Cwmbran’s Grange Hospital where he was later pronounced dead.
“My brother was stabbed about three weeks ago, he was put on medication,” Mr Bashir said.
“He’s been battling mental health for a long period of time.
“The combination of the medication and his mental health, it got a bit stressful.”
FIDDAMAN BLOG
“It’s not about what they tell you, it’s about what they don’t.”
~ Bob Fiddaman, Author, Blogger, Researcher, Recipient of two Human Rights awards
Author of The evidence, however, is clear, the Seroxat scandal.
Citizens Commission on Human Rights Award Recipient (Twice)
Humanist, humorist
Monday, March 08, 2021
Seroxat and the Fallacy of Centrality
Email This
Shane Cooke
Last week, I learned a new term and planned to blog about it. Days later, I read “Gripped by and Discarded by GlaxoSmithKline,” a guest post on Dr. David Healy’s RxISK.org site. This blog explores how the two relate.
Fallacy of Centrality
The term “fallacy of centrality” was coined by Ron Westrum, a researcher who observed pediatricians’ diagnostic practices in the 1940s and 1950s. He found that many of these doctors assumed that they were in a central position, and they presumed if something serious was occurring, they would know about it. If something occurred that they didn’t know about it, well, it just wasn’t happening. This distorted thinking prevented many pediatricians from recognizing and reporting child abuse before the early 1960s. The pediatricians’ applied the “logic” that if parents were abusing their children, they’d know about it.
A present-day example of this type of magical thinking is below (Fig 1). The former head of the Royal College of Psychiatrists, Wendy Burn, uses her “clinical experience” to dismiss SSRI withdrawal. Burn hasn’t seen SSRI withdrawal problems in her practice; therefore, it doesn’t exist or rarely occurs. The fallacy of centrality is problematic among doctors, especially psychiatrists who expose their illogical thinking via social media accounts. It took Burn and many of her colleagues years to belatedly acknowledge the large SSRI withdrawal problem. Their admission came about after many members of the prescribed harm community and a handful of ethical researchers shared the real experiences and scientific facts.
Burn and Professor David Baldwin previously claimed in the national media that “…in the vast majority of patients, any unpleasant symptoms experienced on discontinuing antidepressants have resolved within two weeks of stopping treatment.” (Fig 2) Once again, they embraced the fallacy of centrality.
Fig 1
Fig 2
The same arrogant, illogical thinking is illustrated in “Gripped by and Discarded by GlaxoSmithKline.” It’s the story of a young man, Shane Cooke, who suffered SSRI harms and was later repeatedly victimized by a chain of experts who employed the fallacy of centrality. Shane was just 21 when he decided to leave his foster parents, whom he had been with for nearly 20 years. He became engaged to a young woman, and they agreed to move in together. Both were in their final year at college, which caused understandable stress as they finished their degrees.
Shane was having difficulty eating and sleeping and was anxious about his coursework deadlines. In 2002, he saw his GP, who prescribed two different SSRI brands that precipitated Shane’s suicidality. His GP then switched him to Seroxat, an SSRI sold by GlaxoSmithKline (GSK). Prescribing Seroxat was the norm in the early 2000s given that doctors were not yet familiar with the serious risks the product presents. However, GSK and the British drug regulator, the MHRA, were aware of the problems with Seroxat.
In October of the same year, BBC’s Panorama aired its first of four investigations into Seroxat. Scottish BBC journalist Shelley Jofre extensively reported the problems caused by the so-called ‘wonder drug.’
Prescribing physicians have no excuse for pushing this dangerous and risky drug after this date. Some doctors might argue they never watched the show, but this is a lame excuse. Once again, however, the fallacy of centrality comes into play here: What would an investigative journalist know about a drug that the medical profession doesn’t know?
After being prescribed Seroxat, Shane developed severe agitation, often asking his foster parents, “What’s wrong with me?”
I can relate. The adverse effects I experienced while taking Seroxat and withdrawing from it are documented in my book, this blog, and numerous podcasts.
The full article can be read on the blog These are extracts
Unfortunately, Shane again became a victim of another professional’s fallacy of centrality. . The judge wrongfully assumed that alcohol made “Shane do it.” If a judge has never witnessed violence and alcohol cravings as adverse effects of prescription drugs, the judge decides this simply cannot and does not happen. (It is also true, however, that some judges do know but decide to blame alcohol; it is more convenient and less problematic than blaming a pharmaceutical company’s drug.)
. GSK continues to deny Seroxat causes dependency and suicidal thoughts and actions. However, I do not believe GSK’s false claims are products of the fallacy of centrality.
Today, Shane is active on Twitter and hopes others won’t suffer what he did. Shane and his foster mom, Mary, now run the Prescribed Medication Withdrawal group in Wales.
You can follow him here and read his full story here.
Mary, who is one of the unsung heroes in the advocacy world, can be followed on Twitter here.
The withdrawal group is now doing fortnightly zoom meetings. Anyone within travelling distance of Prestatyn, in particular, are welcome to join in. (this is in the hope of meeting face to face in the future)
You can reach Mary via email at ellen.hennessey@btinternet.com
If you still need convincing that Seroxat isn’t problematic, watch the four investigative reports here. Perhaps you can share them with healthcare professionals who, like so many prescribers out there, probably suffer from a fallacy of centrality.
Petition details
Comments
Updates
Database of those killed or harmed by psychiatric medications and/or diagnoses.
338 have signed. Let’s get to 500!
mary hennessey
mary hennessey signed this petition
Jill Kesti started this petition to World Health Organization and 1 other
This petition was inspired by the Psychiatrist Dr. Yolande Lucire, who writes “A petition needs to go all around the world asking for the signatures of those who have lost loved ones or have had their lives and reputations destroyed.” (by psychiatric medications and diagnoses).
If you or a loved one has been a victim of this failed mental health system, please sign and comment on what happened. Let’s create awareness of those who’ve been harmed. This petition will be delivered to the WHO and the US Federal Government.
Together we can create a better system that actually compassionately cares for and helps people who are struggling. It is time to abandon the medical model of psychiatry and create psychosocial supports for people experiencing distress.
Jill Kesti
Founder of Coalition To End Forced Psychiatric Drugging on Facebook.
http://www.Facebook.com/SisuCreative23
Start a petition of your own
This petition starter stood up and took action. Will you do the same?
Updates
1 week ago
250 supporters
2 weeks ago
Jill Kesti started this petition
Reasons for signing
Scott Norman Rosenthal·2 weeks ago
Psychiatric drugging damaged my life.
3·
Report
Karl Karapetyan·2 weeks ago
I am an advocate of the abolition of psychiatry, both as a medical specialty and an instrument of the law.
3·
Report
View all reasons for signing
Report a policy violation
Sign this petition
Database of those killed or harmed by psychiatric medications and/or diagnoses.
338 have signed. Let’s get to 500!
Jill Kesti started this petition to World Health Organization and 1 other
This petition was inspired by the Psychiatrist Dr. Yolande Lucire, who writes “A petition needs to go all around the world asking for the signatures of those who have lost loved ones or have had their lives and reputations destroyed.” (by psychiatric medications and diagnoses).
If you or a loved one has been a victim of this failed mental health system, please sign and comment on what happened. Let’s create awareness of those who’ve been harmed. This petition will be delivered to the WHO and the US Federal Government.
Together we can create a better system that actually compassionately cares for and helps people who are struggling. It is time to abandon the medical model of psychiatry and create psychosocial supports for people experiencing distress.
Jill Kesti
Founder of Coalition To End Forced Psychiatric Drugging on Facebook.
http://www.Facebook.com/SisuCreative23
Start a petition of your own
This petition starter stood up and took action. Will you do the same?
Updates
1 week ago
250 supporters
2 weeks ago
Jill Kesti started this petition
Reasons for signing
Scott Norman Rosenthal·2 weeks ago
Psychiatric drugging damaged my life.
3·
Report
Karl Karapetyan·2 weeks ago
I am an advocate of the abolition of psychiatry, both as a medical specialty and an instrument of the law.
3·
Report
View all reasons for signing
Report a policy violation
Sign this petition
One of the most EXPLOSIVE revelations from Bob’s blog concerning AKATHISIA written to Dee Doherty from Louis Appleby – a more definitive cop-out you are ever likely to see :
https://fiddaman.blogspot.com/2019/10/uk-suicide-expert-akathisia-can-make.html#.YEo5gCtxc2w
Dear Mrs Doherty
Thanks for replying. I want to try to answer your questions in the most helpful way, so it makes sense to start with my understanding of the main issue you have raised.
SSRI antidepressants can cause akathisia. I have seen many patients with akathisia, caused by different drugs, and it is an extremely unpleasant condition that at its most severe can make people feel desperate and suicidal.
It’s hard to estimate how often it causes suicide or self-harm, partly because what makes people suicidal is often a mixture of problems – it is rarely caused by one thing. However, the risk is sufficiently concerning for us to be cautious at all times, especially when starting or stopping treatment. It’s essential that the doctor who prescribes SSRIs should inform the patient about this risk, as you say, though I do understand that doctors don’t want to put a patient off taking treatment & getting the balanced message of risks and benefits right can be hard.
On the national suicide prevention strategy, I need to explain a little of the background. When we came to update the strategy a few years ago, the Government wanted as few changes as possible. We were keen to add something about antidepressants after hearing from families who felt strongly about this and we thought it was best done in the section on treatment of depression in primary care which was mainly about the risks of getting no treatment. So we added a line to the key messages of this section, as follows:
“There are also risks in the early stages of drug treatment when some patients feel more agitated.” (page 27).
This may not sound a lot but at the time it seemed an important and unusual acknowledgement to appear in a Government strategy. We used “agitated” because it was a document for the general public rather than clinical guidance for doctors – that’s the job of NICE – or information for patients, which is overseen by the regulator, the MHRA. Current NICE guidance says something more specific about the need for careful monitoring in the early period of treatment, especially in younger people, because of suicide risk.
I’m sorry to hear about the difficulties your step-daughter has faced. If she has had severe akathisia on withdrawal, it’s an important point of safety to withdraw more slowly, to avoid the distress I’ve mentioned. Most people can come off antidepressants if it’s done over the right time period, and that can vary for different people.
I hope I’ve answered what you were asking about your step-daughter but if I’ve misunderstood please feel able to come back to me. Of course, I’ve “unblocked” you – happy to do this – but being in touch by email is a lot better than twitter.
With best wishes
Louis Appleby
Cop-in or Cop-out…
“SSRI antidepressants can cause akathisia*. I have seen many patients with akathisia, caused by different drugs, and it is an extremely unpleasant condition that at its most severe can make people feel desperate and suicidal”.
*Life threatening Akathisia can result from the majority of psychotropic drugs, (and other drugs). My caveat.
In view of this above-quoted, apparent recognition, how is is that trainee psychiatrists can achieve specialist accreditation, yet fail to be able to differentiate AKATHISIA from Serious Mental Illness and to misdiagnose as ‘first episode psychosis’?
Why cannot G.P.s (who prescribe akathisia inducing, psychotropic drugs in such abundance) recognise this common, devastating and avoidable ADR, even though most will have had a 6 months psychiatry ‘training’ attachment as part of their 3 years vocational training for General Practice?
The lives lost, or devastated by AKATHISIA IGNORANCE surely could be prevented by addressing what appears to be an unforgivable failure in ‘Specialist Training’, Accreditation, and C.M.E.
Unforgivable. Unaccountable. Unacceptable. Uncompensated. Unrecognised.
‘Depressive psychoses are vanishingly rare compared with treatment induced akathisia’. D.H.
When will they ever learn?
Prescriber awarenesses and concern appears to be the exception. How can consent be valid if the prescriber fails to warn specifically about the risk of akathisia, (and PSSD, and PGAD)?
Tim,
Because it was all hidden in clinical trials as ’emotionally labile’.
Appleby, Wessely, Gerada, Burn, (the latter three having Queen’s Honours bestowed upon them for services for god knows what) have done a major job in the ‘deafening promotion of antidepressants’.
In the UK, where hierarchy is everything, we have a Sir, a Dame, an OBE, who have never stopped trumpeting that the benefits outweigh the risks.
You won’t get far if you look to Psychiatry for reasons why Akathisia is shielded from discourse.
You won’t get far if you look to Pharma-fia as to why ’emotionally labile’ has been so significant in the underplaying.
The half-hearted approach by Burn, latterly, has not resulted in ‘her’ or her ‘Royal’ College disseminating ‘her’ leaflet on Stopping Antidepressants to all GPs and all College Members as a matter of urgency. In fact, Wessely and Gerada have palpably made no remarks on it at all. Zero, Zilch, Nada.
You see, Wendy Dolin and Kristina Gehrki were invited to speak about Akathisia at an RCP Conference and all traces of this have been magically evaporated;
Nemeroff was invited.
https://www.independent.co.uk/life-style/health-and-families/health-news/honoured-britain-us-psychiatrist-who-took-1-2m-drug-companies-8654535.html
Appleby, in contrast, knows all about it.
It is not that Akathisa is unrecognised, it is that all routes lead to the better place that ignoring it can bring..
I will give you an example of how companies like GSK operate.
https://www.msn.com/en-gb/health/medical/new-covid-antibody-drug-reduces-the-risk-of-hospitalisation-and-death-in-some-by-85-25/ar-BB1ews1H
Just look at who is calling the shots here. This is not Seroxat, this is not a vaccine. This is GSK playing the field for all it’s worth and you can bet your bottom dollar that the only people who are making out of this are Moncef Mohamed Slaoui, Patrick Vallance, Andrew Witty, major shareholders, the movers and shakers…
Kim Witczak @woodymatters
The first thing the coroner asked after my husband was found hanging was “what medication was he taking?” She took bottle of Zoloft with her and said “might have something to do with his death.” This was 2003.
So don’t expect any exposé any time soon…
We don’t need ‘heroes’ just professionals properly trained and legitimised to use that skill.
SUBSCRIBE
Lown Institute
How pharmacists can be deprescribing heroes
BY Judith Garber | March 2, 2021
“I am convinced when a single drug is prescribed, the doctor probably knows what to anticipate. When two drugs are prescribed, uncertainty prevails. When three drugs are prescribed, a doctor hasn’t the foggiest notion how a patient will react. When four drugs are prescribed, God doesn’t know what might ensue.”
Dr. Bernard Lown, 2012
We don’t need ‘heroes’ just professionals properly trained and legitimised to use that skill.
SUBSCRIBE
Lown Institute (free to all to subscribe)
How pharmacists can be deprescribing heroes
BY Judith Garber | March 2, 2021
“I am convinced when a single drug is prescribed, the doctor probably knows what to anticipate. When two drugs are prescribed, uncertainty prevails. When three drugs are prescribed, a doctor hasn’t the foggiest notion how a patient will react. When four drugs are prescribed, God doesn’t know what might ensue.”
Dr. Bernard Lown, 2012
This is the first time that details of exactly what happened to Shane on Seroxat have been shared in print by us. The daily papers used their own versions at the time – but we all know how long those reports last in the public’s mind : just until the following day’s edition. Locally, everyone knew – the recurring visits by police and ambulances kept his condition uppermost in everyone’s mind. That was many years ago now. With the recent post on Rxisk, a new set of people, who supported our attempt to establish a local withdrawal group, have been introduced to the details. Much horror and utter disgust has been expressed that so little help was available from the “services” in Shane’s ‘hour of need’. These are people who attended both meetings that we had with David in Prestatyn, who were shocked by the facts that David shared with us on both occasions. However, reading about the actual suffering of someone that they know has stirred an even deeper realisation of exactly what these drugs can do – and STILL do. Shane is one of many, and may be the only one in our corner of Wales, to suffer in quite such a dramatic way. For this reason I really feel that these reports need to be brought TOGETHER in a way that could be handed out in our localities in order to keep alive the relevance of our struggle for informed consent and full knowledge of the state of mental healthcare in our areas.
I remember going with Shane to a GP appointment soon after his return home. It was not with his named GP but another regular at the surgery. The GP’s screen was full of the details of all that had happened, of course, and his words when he turned to Shane were : “I’ve been telling them here for a long time that these SSRIs can cause havoc for some patients – maybe they believe me now!”
Whenever we encounter a setback, with whoever may be trying to silence us, it is important that we keep going – keep reminding others that we know from experience exactly what can happen to anyone given a prescription without an understanding of the unexpected demons that could come with it.
DR YOLANDE LUCIRE
Adverse Drug Reactions
Attention: Health Ministers
Psychiatry, Pharmacogenetics, & Adverse Drug Reactions Research
In 1942, the Polish resistance fighter Jan Karski gave
eye witness testimony to the Supreme Court judge Felix
Frankfurter of the clearing of the Warsaw Ghetto and the
systematic murder of Polish Jews in the Belzec Concentration
Camp, listening to him, Frankfurter, himself a Jew, and
one of the outstanding legal minds of his generation replied,
“I must be frank. I am unable to believe him.” He added,
“I did not say this young man is lying. I said I am unable
to believe him. There is a difference.”
What explains our ability to separate what we know from what we believe, to put aside the things that seem too painful to accept?
How is it possible, when presented with overwhelming evidence – even the evidence of our own eyes – that we can deliberately ignore something, while being entirely aware that this is what we are doing?
This inability to believe applies to everything else that is unthinkable, such as what we see in front of us; that we are causing depression, suicide, and death by the injudicious and careless use of psychiatric drugs in persons who are having normal human reactions to life stresses.
Tuesday, June 2nd, 2015
SSRI Ed note: Many people have reduced or no ability to metabolize SSRIs due to a deficiency in CYP2D6 (cytochrome P450 2D6), an enzyme needed for 1/4 all prescriptions.
To view original article click here
Investment Watch
by IWB
June 2, 2015
More than a decade ago, Dr. Yolande Lucire started noticing high rates of hospital admission and suicide among patients treated with antidepressant medications and antipsychotics.
Almost another decade later :-
Database of those killed or harmed by psychiatric medications and/or diagnoses.
342 have signed. Let’s get to 500!
This petition was inspired by the Psychiatrist Dr. Yolande Lucire, who writes “A petition needs to go all around the world asking for the signatures of those who have lost loved ones or have had their lives and reputations destroyed.” (by psychiatric medications and diagnoses).
BMC Medicine
Part of Springer Nature
Open Access
Published: 15 July 2020
Safety of psychotropic medications in people with COVID-19: evidence review and practical recommendations
recovery&renewal Retweeted
Dr Ed White
@Reduxreloaded
·
2h
This is very sad to hear. You have put an amazing amount of effort into raising awareness of a hideous issue. I’m sorry to see you go, but fully understand your reasons.
AntiDepAware
@AntiDepAware
5h
I have decided reluctantly to end my involvement with the AntiDepAware website. Although the site will remain online, there will be no further updates, and the email address is no longer valid. Many thanks to all those who have contacted me and given me encouragement.
May I send my warmest best wishes and thanks to Brian for his immense amount of critical work.
FOI Requests (Cardiff and Vale UHB – Information Governance), The Yellow Card Centre Wales 15 March 2021
Freedom of Information Act 2000 – Request Reference FoI/21/102SSRIsRequest DetailsCan you please let me have information regarding reports of adverse effects to SSRIs including suicides during last 2 years.
After reminding them that the response was overdue – this is how Wales handles FOI requests despite making a big huha to encourage people to get involved. Obviously I was not expecting anything much but at the least this mirrors the laziness and uselessness of the Welsh arm of the MHRA
Response DetailsAfter considering your request, Cardiff and Vale University Health Board (the UHB) believes that Section 21 of the Freedom of Information Act 2000 applies in this instance and is refusing your request. The reason for relying on this exemption is set out below.Under Section 21 of the Act, an organisation does not have to respond to a request if the information being sought is reasonably accessible to the applicant by other means. The UHB has applied this exemption to your request as the information you are seeking is available in the public domain. Under our Section 16 obligation to advise and assist, I can confirm that the relevant data can be found by clicking on the following link;https://yellowcard.mhra.gov.uk/idapThe UHB would also like to advise you that it is not the Data Controller for yellow card data and that, should you wish to obtain additional information, this may be available by contacting the MHRA (Medicines and Healthcare products Regulator
I was told they were the responsible org. and in the first reply to my letter did not disagree that was the case
Extract from Welsh YCS promotion :- have sent them a copy as they don’t seem to understand their own role
The Yellow Card Centre Wales
YCC Wales is one of five regional adverse drug reaction monitoring centres, acting on behalf of the Medicines and Healthcare products Regulatory Agency (MHRA). YCC Wales has a vital educational and communicating role to encourage suspected adverse reaction reporting via the Yellow Card Scheme (spontaneous reports of suspected adverse drug reactions) to both patients and local health professionals in Wales.
Staff of the Centre have lectured, held workshops, poster presentations and seminars on pharmacovigilance to encourage the spontaneous reporting of suspected adverse drug reactions from both healthcare professionals and members of the public. They have continued to explore other mechanisms to encourage reporting.
A strong safety culture requires good reporting of adverse events and critical incidents. It is encouraging that the reporting rate for suspected adverse drug reactions via the UK Yellow Card scheme in Wales was 50% higher than for the UK as a whole in 2010 (30.5 vs 19.7 reports per 100,000 population). One of the reasons for this high reporting rate is the result of concerted efforts by health professionals, led by the Yellow Card Centre Wales and supported by the All Wales Medicines Strategy Group (AWMSG), to educate colleagues and future health professionals concerning the importance of reporting of suspected ADRs.
More blah – or an opportunity ? (I haven’t a clue how to use a webinar – think pyment is involved)
Webinar on Research integrity: how can we support and protect early-career researchers in cases of scientific misconduct?
Please join our webinar on 22 March at 15:00 CET titled ‘Research integrity: how can we support and protect early-career researchers in cases of scientific misconduct?’. This webinar will be organized by the YAE in collaboration with Academia Europaea, SAPEA and the European Group on Ethics.
The event is open to everyone and will include a Q&A session, where the audience will be able to interact with the panelists. During the webinar several questions will be addressed, including: ‘What processes are in place to address potential problems of malpractice?‘, ‘What actions might be taken, at individual, institutional and government levels to facilitate the process of investigation and, where necessary, protect those involved?‘.
If you are interested in answering the above and other questions, join the free webinar by registering here:
To find out more, visit the Academia Europaea’s website.
BBC 1 9pm,a documentary about Male suicide involving young men. The programme was presented by Ronan Kemp a popular UK celebrity, who had lost a close friend to suicide. No real reasons as to why this happened were explored. The fallout for those left was addressed. Then Ronan starts stating almost as fact.that Sertraline really helps him, his been on it since he was 15,(He is now 27) if if doesn’t take it for a couple of days the chemical imbalence comes back. Quote for me it’s Dr’s and Meds. This is an outrageous message in 2021,has the BBC become Pharmas Pimp? Why is this narrative not challenged? No doubt Twitter will be ablaze tomorrow and critics will be accused of pill shaming. Umm wonder if Ronan has sexual dysfunction…. If he admitted that, to his army of young followers that may indeed Provoke a much needed discussion about Men’s MH and reasons behind completed suicides…
FROM KATINKA BLACKFORD NEWMAN:
RECOVERY STORIES – for those of you that don’t know me, I’m a psychiatric survivor and also run a campaign (www.thepillthatsteals.com) to warn people about the dangerous side effects of antidepressants.
I’m starting a new campaigning website to replace the old one and I’m looking for Recovery Stories. If you’ve been on a number of antidepressants/antipsychotics, suffered side effects, withdrawn and subsequently got your life back I’d love to hear from you. I need a photo and up to 1500 words – alternatively I can talk to you on the phone and write your story. Please write to me at Katinka.Newman@gmail.com
With thanks
Know Your Drugs