
Could It Be Intelligent to Say No?
The meat in this post comes from Peter Selley and centers on a new hazard of monoclonal antibodies given to infants – seizures and other neurological problems, along with deaths. The background to this post lies in Ground Control to RSV – RSVP.. It also links to Back to the Future of Personal Care on RxISK.
In The Miracle of Artificial Intelligence, David Healy outlined a conversation about A. I. with 4 well-educated, on-the-ball, professionals in their early 30s – the new child bearing age bracket. They were A.I. enthusiasts and likely too young to have ever heard of Nancy Reagan’s Just Say No.
Did you use A.I. in deciding whether to give your prospective newborns Abrysvo when in the womb or Beyfortus (nirsevimab), a monoclonal antibody, immediately after birth to provide protection against RSV? Yes.
What did A.I. say? It was a no-brainer. We absolutely should get him/her protected. And everything worked out fine? Yes. No problems.
In April 2024, Chile became one of the first countries in the world to roll out universal RSV coverage with Beyfortus. The Chilean RSV (Respiratory Syncytial Virus) season is from April to September with a peak in June and July. Did the data from the first RSV season live up to the promise and would it reassure our current child-bearing researchers?
Asking A.I.
Q. What were the results of the Beyfortus roll out in Chile.
-
Reduced RSV Hospitalizations:
The implementation of the nirsevimab immunization strategy in Chile led to a significant decrease in hospitalizations for RSV-induced lower respiratory tract infections (LRTI).
-
Lower Severe Cases and ICU Admissions:
The program also reduced the number of severe cases requiring intensive care.
-
Impact on All-Cause Hospitalizations:
The public health impact extended beyond RSV, with a notable reduction in all-cause LRTI hospitalizations observed.
-
Reduced Healthcare Strain:
The strategy eased the burden on the healthcare system, decreasing the demand for emergency room visits and hospital beds during the peak RSV season.
-
Cost-Effectiveness:
The roll out was found to be cost-saving, particularly by reducing direct patient costs, making it a viable and beneficial strategy for the Chilean health system.
-
High Immunization Coverage:Chile achieved high coverage rates for the Beyfortus vaccination during the campaign, indicating successful uptake of the new preventive measure among the target population.
We can add to this. As published in the Lancet, Results of the first season were impressive – there was a more than a 94% uptake and, remarkably, no infant eligible for nirsevimab died due to RSV infection, compared with 13 deaths reported in 2023.
145,087 babies were Beyfortified, and with only 18 reported adverse events (0.012%) that might have been attributed to the antibody/immunisation, but were not directly attributed to it – not even “injection site pain”.
RSV-related-LRTI-hospitalisations in immunised infants were reduced by 76·41%.

This August 29 2025 tweet on X celebrates this. There are uncanny echoes here. Fifty years ago Augusto Pinochet began implementing the proposals of a group of Chicago trained Chilean economists to his government, setting in motion what is now called Neo-Liberalism.
More Questions for A.I.
We can also ask A.I. Are there any risks from Seizures following Beyfortus or Enflonsia (clesrovimab – the latest monoclonal) ?
Q. What is the seizure risk with nirsevimab (Beyfortus)?
- The available evidence suggests the seizure risk with nirsevimab (Beyfortus) is very low, aligning with the expected background rate in infants rather than being directly caused by the drug. While isolated cases have been reported, comprehensive safety data from clinical trials and post-marketing surveillance indicate a favorable safety profile for nirsevimab.
- Post-marketing data from Spain’s 2023–2024 immunization campaign found that serious adverse events peaked early in the program, which is typical for new medications.
[Comment: In this Spanish so-called study, no seizures were reported amongst the 67 children who apparently had Serious Adverse Events out of 277,000 immunised with nirsevimab.]
A.I. Updates?
The question is when will A.I. catch up, if ever, with the second Chilean RSV season, which is just coming to an end.
Instead of RSV infections dwindling, there has been a late outbreak with RSV Isolations 50% Up on the equivalent week last year. There has been a sustained rise in all types of respiratory infections and paediatric critical care bed occupancy exceeds 80% nationwide.
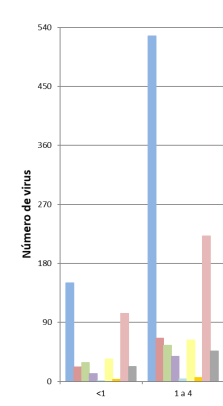
The blue column is RSV. The orange column on the right is Rhino virus. The yellow column in the middle is Metapneumonia. The others are Parainfluenza, Influenza A and B, Sars-Cov 2 and Other Respiratory Viruses.
There are also data for the elderly in the link above. This data might have interested the Pope who because of his compromised lungs got the Abrysvo vaccine and succumbed to a complex respiratory problem later on which seems to have been complicated with Meta-pneumonia, an infection that RSV infections protect us against.
The data of real interest affect 1-4 year olds. Could these data have been foreseen – Yes. Was A.I. likely to foresee them? Almost certainly not.
With Covid lockdowns, infants and children kept at home didn’t get RSV as per usual in the first weeks of life. When lockdowns were lifted, children caught RSV later than they usually do and it appears to be more severe when caught later.
What seems to be happening is that the monoclonal antibody – Beyfortus or Enflonsia (below) does not provide the enduring protection that a natural infection offers. This is bad for us but good for business – it opens the door to an annual pre-RSV season jab.
It’s uncannily like an SSRI company positively welcoming the fact that you can’t get off their drug.
What about neurological problems linked to monoclonal antibodies given to infants?
Meddling with babies
The Medley trial was AstraZeneca-Sanofi’s non-inferiority randomised controlled trial comparing nirsevimab (Med18897– Beyfortus) with an off-patent monoclonal antibody palivizumab in preterm babies and babies with congenital heart or lung disease (CHD-CLD).
The results were published as a NEJM “special”. A Long letter to the journal, longer than a doctor or academic would be allowed. Letters dodge the peer review normally expected for clinical trial results.
The letter claimed “The incidence of adverse events was similar across treatment groups”.
But “Five deaths occurred in the nirsevimab group and One death occurred in the palivizumab group. All deaths were thought to be unrelated to treatment by the investigator.”
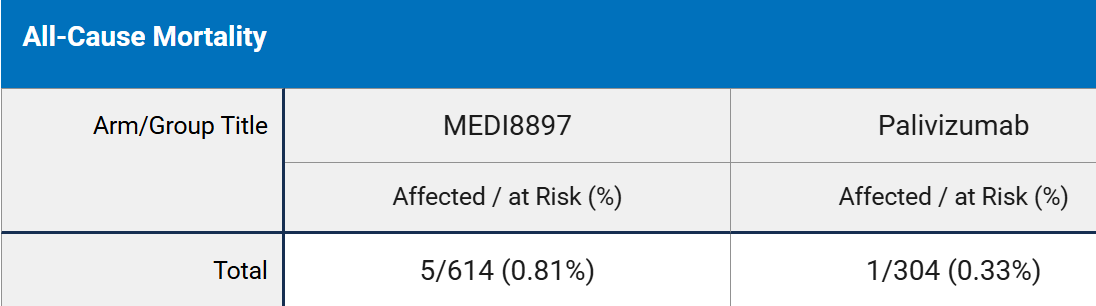
Now some of us might think that a death rate of 0.81% in the nirsevimab group is “similar” to 0.33% in the palivizumab group but some soon to be parents might wonder “Isn’t that more than twice as many?”
Until 2018 Palivizumab was an old and expiring AstraZeneca product. It was only given to vulnerable children – those who had serious problems or were very premature. AstraZeneca offloaded it after its patent expired and nirsevimab came along.
The aim of the trial was to show a single dose of nirsevimab was non-inferior to palivizumab as regards safety. It is not clear there is any scientific reason to ditch palivizumab in favour of nirsevimab. There was however a clear financial reason to switch and roll out a bandwagon – give it to all infants in order to reduce hospitalizations and save health services.
Would you expect A.I. to report on Nirsevimab as the NEJM Long Letter reports on it or do you expect A.I. to be able to discern what some party-poopers claim is really going on?.
Death Defying
What about ditching palivizumab or Beyfortus in favour of clesrovimab Enflonsia – the new kid on the block? Enflonsia is another monoclonal antibody controversially approved by the new-look Advisory Committee on Immunization Practices (ACIP) for FDA in June.
Merck (like other pharma companies) normally likes to show the relative benefit/risk of their product. In this case there are 100% more deaths in the clesrovimab group when compared with palivizumab and its a much better bet to report the difference in deaths as an absolute difference in the percentage i.e. 0.9% more deaths in the clesrovimab group.
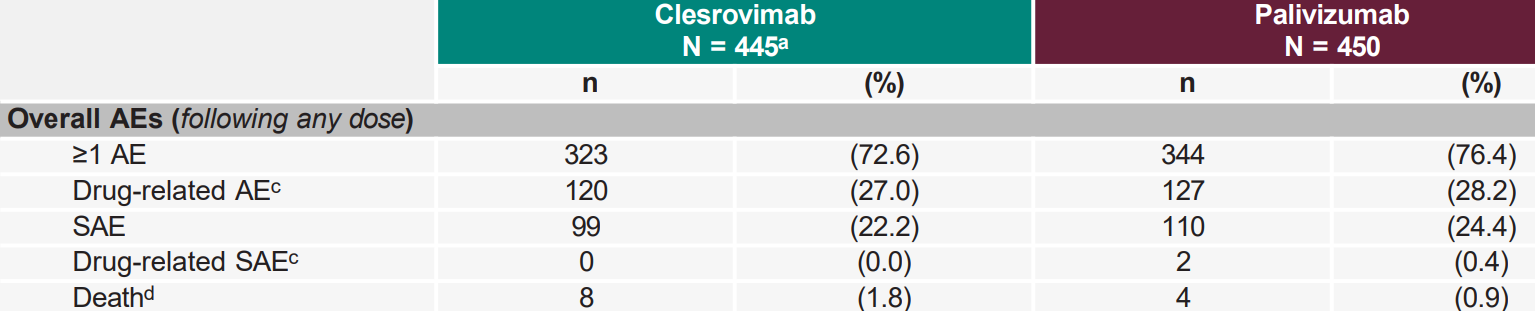
What’s 0.9% between friends.
Merck concluded:
- Clesrovimab was well tolerated in infants at increased risks for severe RSV disease – in season 1, the safety profile of clesrovimab 105 mg was generally comparable to that of palivizumab
“Similar” and “Comparable”. 4 is similar to 8 and a sports car is comparable to a jalopy.
Seizures
Generally Comparable or Similar is a motif running through all assessments of the RSV monoclonal and vaccine data. In an earlier presentation to ACIP on nirsevimab, the Vaccine Safety Division linked to the Centers for Disease Control and Prevention (CDC) said that in clinical trials “adverse events were “generally balanced” versus comparators among infants.
FDA’s integrated review of nirsevimab had commented on and dismissed an excess of deaths as similar. It made no mention of the neurological problems – especially seizures, convulsions – which do not look so similar in the table below. (‘NIRS’ is nirsevimab, ‘PBO’ is placebo.)
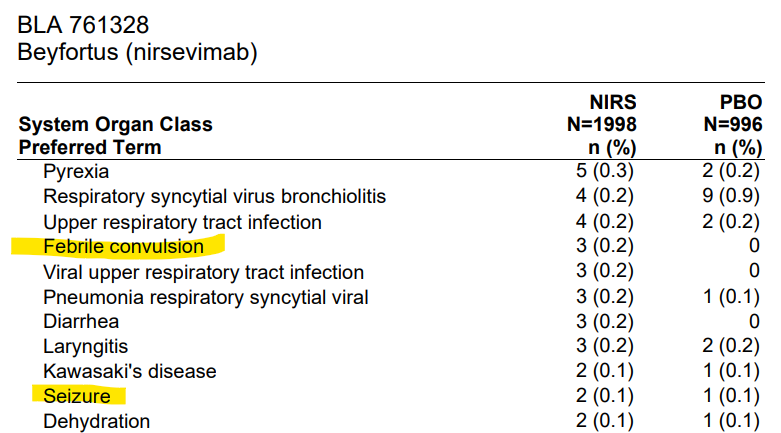
The highlighting here seems to have been done by CDC – for some unexplained reason. The table also omits status epilepticus and likely other events that show up with Enflonsia below.
When analyzing the seizure risk in nirsevimab trials, the Vaccine Safety Division made some strange moves and then claimed the risk of “seizures” was similar to, or comparable to, or balanced between nirsevimab and placebo.
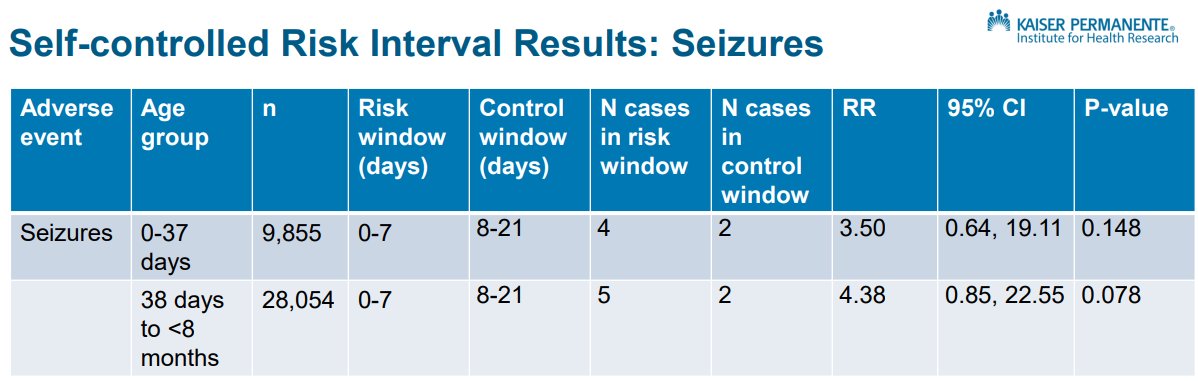
In the absence of a clear reason to split the first week post Beyfortus into two groups – under and over 38 weeks – this looks like an attempt to produce two groups neither of which is statistically significant. Amalgamate the groups – all first weekers post injection with those in the following 2 weeks and the results are statistically significant.
But even without amalgamating the data here, there is clear evidence of a problem and the company could warn but hasn’t – companies don’t have to have statistically significant data to warn – as FDA have been telling them for 3 decades since the SSRIs had a clear excess of suicidal events on active treatment compared to placebo. Companies – not FDA – chose not to warn figuring they can win in court by claiming the safety data do not show a statistically significant hazard.
In the current climate if a benefit is demonstrated FDA have little option but to approve and Beyfortus was approved as clesrovimab (Enflonsia) has been more recently.

Enflonsia’s Serious Neurological Adverse Events were reported in a Merck RCT comparing 105mg of clesrovimab (a huge dose) to saline placebo (right).
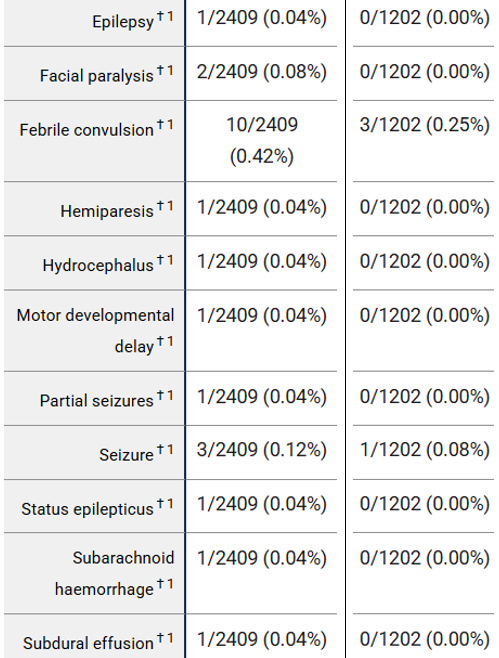
A serious adverse event (SAE) is one that results in death, a life-threatening adverse event, requires inpatient hospitalization or prolongation of existing hospitalization, a persistent or significant disability or incapacity.
Would any parent run the risk of their healthy baby having events like these for the sake of some protection against a mild illness?
What about the 2/2409 instances of “facial paralysis” in healthy babies given clesrovimab? Facial paralysis (which includes Bell’s Palsy) is a fairly rare condition, where one side of the face is paralysed. In children, acquired facial paralysis is extremely rare (2.7/100,000 annually in those <10 years of age, and even rarer in babies, where most cases arise from trauma during birth). These two cases occurring after immunisation should make clinicians’ ears prick up. Facial paralysis may be a manifestation of Guillain-Barré syndrome.
One of our options through out politicians or doctors are to demand information on the risks from companies who do not show the details of what happened these babies. The other option is to Just Say No. Our doctors help with this would be good to get – but they get paid for giving vaccines or injections like this.
Current regulatory systems are configured as CDC’s GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) assessment template shows:
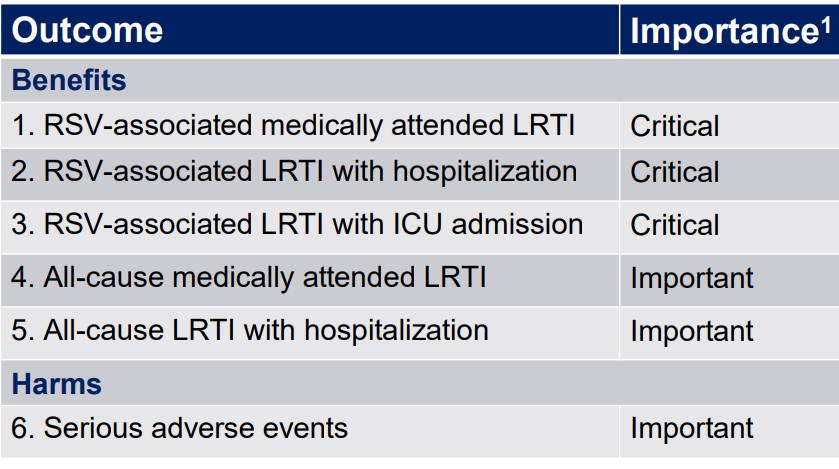
Once a benefit has been demonstrated, FDA, CDC, and ACIP etc have little option but to approve. Companies write the label which centers on the promise the treatment offers and can opt to spin any serious consequences as comparable or similar to placebo – in the Shit Happens domain – so rare you’d be most unlikely it will happen to fit, young, smart, elite, A.I.. using professionals like you.
With Enflonsia, the 105 mg dose given to a newborn is the only available dose and is huge. Beyfortus has both a 100 mg and a 50 mg dose. This is supposedly for over and under 5 kg weight babies.
Could FDA have asked for an analysis of serious Enflonsia adverse events depending on dose by suggesting analysis by babies weight? Lighter babies are getting a much higher dose of an already high dose. Perhaps they could but the results would almost certainly have ended up described as generally similar or comparable.
This is not a new state of affairs, nor is it evidence of FDA ‘slipping’ and keeping us less safe than they once did.
Heading toward 4 decades ago, they were faced with the exact same scenario with Prozac (Fluoxetine) and Paxil (paroxetine) being brought on the market at 20 mg, the very top of the dose range for an SSRI. It is almost for certain the higher dose of these drugs caused more suicides, homicides, severe withdrawal and other problems than a lower dose would have done – and there were 5 mg trials of fluoxetine showing it to have just as good efficacy as 20 mg.
But Lilly then, and perhaps Merck now, wanted to keep life simple for busy doctors with a single dose.
FDA do not have the power to force companies to run further low dose trials. FDA is not there to put a brake on company behavior, other than curtailing wild claims that have no data to support them.
When the system was set up, there were two brakes on company behavior. The first was the power of professional organizations to Say No unless a treatment’s label and other information was responsible. But these brakes have worn thin and would no longer pass muster in a road safety test.
The fallback brake is/was our ability – in the US but not elsewhere – to sue companies for injuries and a failure to warn. These are getting pretty thin as well. Who cares about the brakes – look at this gorgeous Eve sitting on the bonnet of what is about to be your new sportscar.
Getting to Yes

If Nancy and Ron had been in the Garden of Eden rather than Adam and Eve we might have been saved a lot of grief.
In Eden all our Needs were provided for. But beyond Needs we have Wants and here is where temptation comes in. A promise. A promise without consequences.
This is where company marketing comes in. Assisted increasingly by A.I., it aims at Getting Us to Yes.
In parts of the Global South there is perhaps a Need for RSV vaccines or monoclonals. For those of us in the developed Eden, there is no Need for these. Things can only go wrong.
But creating Wants and catering for them – because We’re Worth It – can seem to give Smart People like Us a purpose in life. Banishment and Exile from Paradise – wasn’t that a fairly-tale?
This post links inseparably to Back to the Future of Personal Care on RxISK.org.
Serious Adverse Events and Seizures
WHO has guidance on reporting adverse events after immunisations
https://iris.who.int/bitstream/handle/10665/340802/9789241516990-eng.pdf
They say that adverse events should be reported within “a plausible time window” with no further explanation. Commonly this period ranges from 10 – 30 days after immunisation.
(For example this would have excluded the two boys who died of enhanced RSV chest infections about a year after their vaccinations in 1966.)
https://undark.org/2023/10/09/rsv-vaccine-children-trials/
About 2 out of 10,000 babies have seizures in their first year of life, often associated with a fever – so-called febrile convulsions. Seizures in infants are normally classed as serious and usually result in hospital admission.
It is not credible that there was not a single seizure reported in the of 277,000 Spanish children after immunisation with nirsevimab, where one would normally expect there to be about 55 episodes. Similarly in the study in 145,087 babies in Chile, four adverse events were reported as serious and 14 were non-serious. There was only one seizure reported whereas 29 would have been expected.
These “real-world” data post marketing trials are surreal: the results are completely different to the outcome of the “gold standard” clinical trials seen by the regulators.
Peer review has become an embarrassment.
Veering slightly away from RSV; Nancy and Ron, the politicking – peer review
“Clear Factual Data”
American Psychiatric Association@APApsychiatric Aug 28
IMPORTANT: Decades of rigorous research, randomized clinical trials, peer-reviewed studies, meta-analyses, national registry studies, and FDA oversight show that psychiatric medications are safe and effective. Medications like SSRIs can be lifesaving if they are taken as directed under the care of an appropriately licensed healthcare professional.
Learn more: https://ow.ly/RWEQ50WNJeI
Kim Witczak @woodymatters
Internal FDA memo (1991) on Zoloft — released in my litigation vs @pfizer
https://x.com/woodymatters/status/1961633266055762144
Will flattery to DJT, get Pfizer everywhere..
https://on.pfizer.com/3I1wl8A
To date, data on Pfizer’s COVID-19 vaccine have appeared in over 600 peer-reviewed publications.
‘Such an accomplishment would typically be worthy of the Nobel Peace Prize, given its significant impact.
President Trump’s call for transparency is welcomed, and we remain deeply committed to that principle. Transparency has always been a cornerstone of trust, and we are dedicated to continuing to provide clear, factual data to the public.’
Annie,
For those who have suffered fatal and life-long grievous bodily harm; and psychological, social and economic devastation from psychiatric drugs enforced for misdiagnosed AKATHISIA ‘by an ‘appropriately licensed health care professional’: – your quoted ‘IMPORTANT’ statement claiming ‘safe and effective’ appears to be misleading..
For all those injured by the cavalier and injudicious use of such toxic drugs; reading is painful.
Surely this would not fulfil acceptable U.K. standards of medical communication to the public?
GMC: – Professional Communication. 89. You must make sure any information you communicate as a medical professional is accurate, not false or misleading. This means:
b) You must not deliberately leave out relevant information.
c) You must not minimise or trivialise risks of harm.
I appreciate that your link gives access to a more extensive publication, but the paragraph you have copied is surely scientifically questionable?
“The greatest enemy of knowledge is not ignorance, it is the illusion of knowledge”. Stephen Hawking.
Tim
IMPORTANT:
My reply to Peter was about peer review and his view that it is embarrassing, and I gave two examples. The first one was from the American Psychiatric Association, who quoted ‘peer-reviewed studies.’
I followed this with a tweet from Kim Witczak, which was in reply to the APA. Kim’s full tweet, with the APA at the top, was in reply to the APA. It is sometimes the case that in a tweet you have to scroll up to see why they have tweeted what they did and you can see this from the position of the side-bar.
Kim Witczak @woodymatters ·Aug 30
Replying to @APApsychiatric
https://x.com/woodymatters
Of course the APA is scientifically questionable, that was the reason Kim replied as she did, and we all know the APA is very wrong-footed.
Your points are valid and correct. The APA is indeed ‘painful’ reading for all of us harmed by SSRIs
and I apologise that you found it to be ‘misleading’. Kim replying to the APA as she did and all her work, from her tragic loss of Woody, is outstanding.
Annie,
I’m sorry that my words may have suggested that I found your comment misleading.
It certainly is not, and as always, your comments are sincerely appreciated and respected.
I thought that the entire “What is a psychiatrist”? APA promotion of their Guild was beyond propaganda, and apparently deceptive, when alleging psychotropic drugs are “safe and effective”.
Tim.
Thanks, Tim
If either of these two things happen, then the APA, Etc., will look pretty foolish and inept.
Previously posted on Lonesome Heroes can work Miracles on Rxisk.org
RFK Jr “We’re launching studies on the potential contribution of some of the SSRI drugs and some of the other psychiatric drugs that might be contributing to violence.”
Amid cries for retraction, a medical journal reviews a discredited, 24-year-old paper on an antidepressant
The Journal of the American Academy of Child & Adolescent Psychiatry is reviewing a study of Paxil
https://www.statnews.com/pharmalot/2025/08/25/antidepressant-paxil-gsk-medical-journal-children-adolescents-depression-ghostwriting-retraction/
Also on Rxisk.org
Dr. David Healy says
September 1, 2025 at 8:08 pm
Merrill Goozner from Gooznews has published a hard-hitting comment in early August I missed
‘The 10-person roster, seven of whom were men, was larded with critics who have spent their careers attacking the science behind anti-depressants and questioning their use, both in pregnancy and in general psychiatry. They included David Healy, the British physician who has written books attacking the use of seritonin reuptake inhibitors (SSRIs) in particular (the subject of the hearing), and has served as a paid consultant for trial lawyers suing the companies that make Prozac, Zoloft and Paxil.’
Lard and lah di dah
It is important to follow things, closely..
A rally this Tuesday in Vienna to relaunch the investigation into Romain’s suicide in 2021. The family from Nord-Isère denounces the adverse effect of antidepressant treatments on their son’s behavior
https://www.bfmtv.com/lyon/videos/video-un-rassemblement-ce-mardi-a-vienne-pour-relancer-l-enquete-sur-le-suicide-de-romain-en-2021_VN-202509090234.html
Vienna: a family mobilized against the negative effects of anti-depressants
https://www.rcf.fr/actualite/focus-isere?episode=611239
Four years ago, Romain Schmitt, then 17 years old, from Isère, committed suicide. For a few months, he had been taking an anti-depressant, and his behavior had changed radically. Mood disorders, catatonia attacks… Symptoms, classified as side effects of paroxetine, as well as suicidal thoughts, especially in young people. Since then, her parents, Yoko and Vincent, have been fighting to shed light on these little-known effects of the “happiness pill”.
Especially since Romain is not the only victim, according to Ariane Denoyel, a Grenoble journalist and expert on the subject: “We can estimate that there are tens of thousands of victims.
I’ve been grilling Grok. Daring to tread where no scientific illiterate has trod before.
My question. The big message I’m getting from Dr Selley’s analysis is that the ‘passive immunity’ conferred by Beyfortus, may actually be interfering with vaccinated infants’ development of natural immunity. This could be one explanation for the rise in RSV cases in Chile – and a longer-term undermining of the health economics of vaccination against mostly mild disease in rich countries. What do you reckon?
A. Current Evidence: Dr Selley’s report cites a 50% increase in RSV isolations and 80% paediatric occupancy, contrasting with 2024’s success (76.41% hospitalization reduction, no deaths, 0.012 adverse events in 145,087 infants.)
No data specifies whether 2025 cases were in previously immunized infants, older children, unvaccinated groups nor whether severity increased. If the surge involved Beyfortus with waning immunity it supports your hypothesis.
Adverse Event Reporting and Antibody-Dependent Enhancement (ADE)
Current evidence: Chile’s 2024 ADE rate (0.012, 18/145,085) is lower than Spain’s 0.024 and trial rates (1-2% SAE) suggesting underreporting of mild event or stringent criteria.
Testing your hypothesis; without longitudinal immunity studies or 2025 Chilean case specifics, we can’t confirm if Beyfortus passive immunity caused the surge by delaying natural infections. The Lancet modelling support the possibility but real-world evidence is lacking.
The Lancet Regional Health- Europe (2024) suggests passive immunity from Beyfortus may shift RSV infections to older ages (1-2years) potentially increasing susceptibility if natural immune responses are delayed. However, no studies measure whether Beyfortus suppresses active immunity (e.g. B/T cell responses) or increase later infections. Palivizumab, an earlier monoclonal antibody, showed no significant immunity suppression, but it was only used in high risk infants.
I also tripped over this Spanish authored article –
‘Second-season Impact of Nirsevimab: Clinical Outcomes of RSV Disease in Patients Immunized During Their First Season’ – confirming the concern about antibody dependent enhancement. Commonsense – mess with infants’ naturally acquired immunity and what happens?
byhttps://journals.lww.com/pidj/fulltext/9900/second_season_impact_of_nirsevimab__clinical.1415.aspx
‘Nirsevimab provides passive immunization against respiratory syncytial virus, yet concerns exist regarding its long-term impact. This study analyzed respiratory syncytial virus-associated lower respiratory tract infection severity in hospitalized children immunized with nirsevimab more than 6 months prior. No significant differences were found compared with nonimmunized children. Findings suggest no increased risk in the following season, supporting nirsevimab’s safety as a preventive strategy.’
What struck me as curious is that the unvaccinated sample they were comparing the nirsevimab jabbed babies with was hugely biased towards premmies or those with chronic diseases, littl’uns who were more likely to have needed prior hospital admission. So how impressive is it that the nirsevimab sample were doing no worse than them?
I’ll leave those of you with the scientific minds I will never have to make some sense of this.