See below for an explanation of this image.
Will Powers work on Post-Finasteride Syndromes (PFS) has generated a lot of interest. It would be easy to misread the responses.
This post asks people with PSSD and PAS to get what are often called Dutch tests done. The U in Dutch stands for Urine.
Can send your results to david.healy@rxisk.org – not to Dr. Powers. He was swamped even before the recent Congress and is even more swamped with desperate people getting in touch unaware of the extent to which he is badly over-stretched.
This ask does not apply to Finasteride. Enough material has already been collected by or sent into Dr Powers for Finasteride. His next step involves trying to figure out if the results he already has provide a basis for testing possible remedies – something that will undo the metabolic road-block people with PFS seem to have,
Will and RxISK are on the same page in viewing the enduring sexual dysfunctions as feedback loop disorders – See Enduring Sexual Dysfunction and Love Making Actually. This is not an effort to divert people away from Will – it’s an effort to avoid him burning-out. We will be depending on him to shape any interpretations of the data being asked for here.
Dutch and Double Dutch Science
The response from researchers and mainstream medicine to the idea that Will’s work depends in part on Dutch Tests is that these are barely respectable tests likely to tell us little more about what is going on in people than reading the urinary output of the Kremlin or the Pentagon. I had never heard of Dutch Tests 3 weeks ago.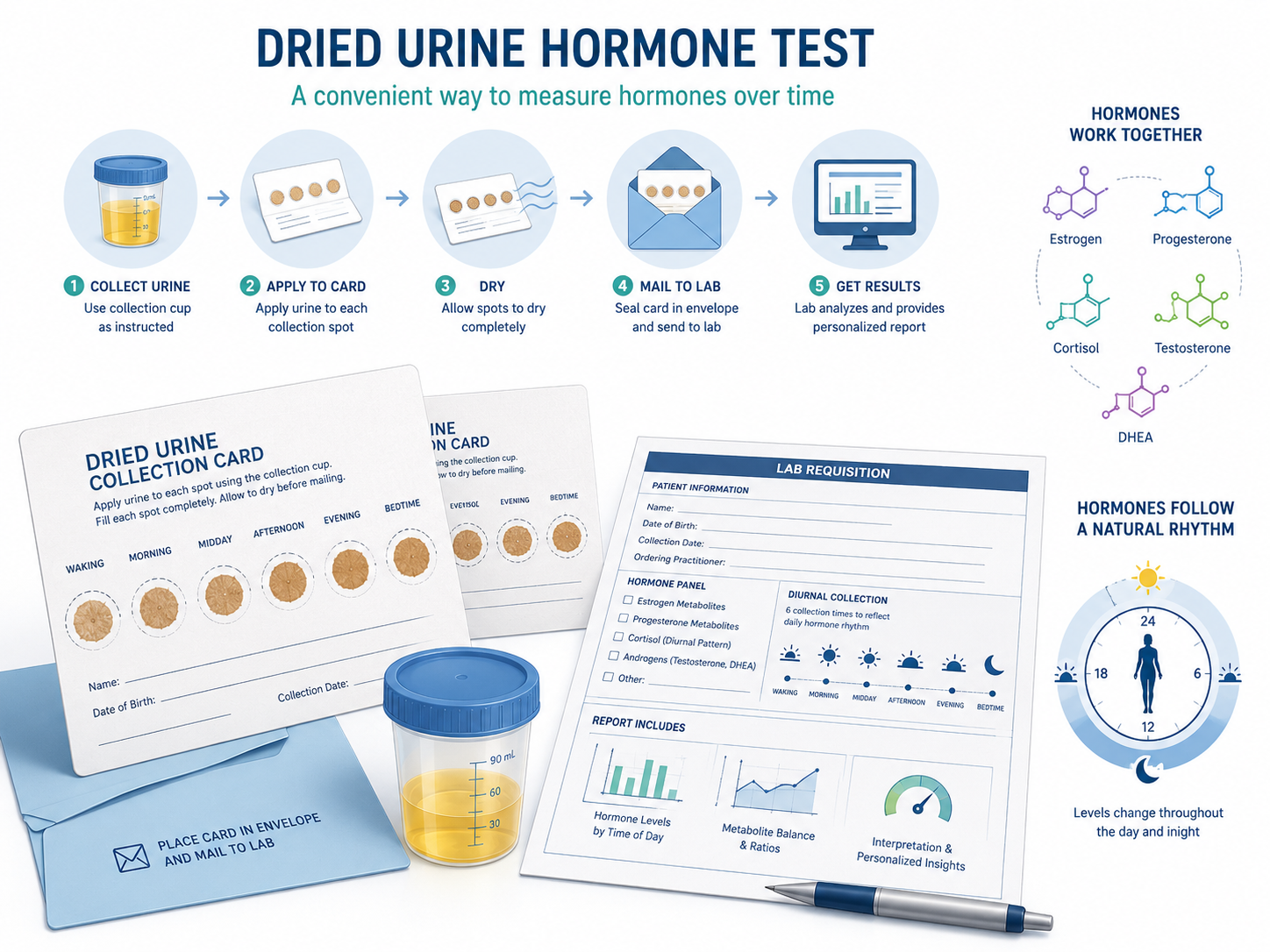
A skeptical response is normally right but misses the sequence of events here. Will didn’t start with Dutch tests. He began interpreting genomes where he noticed a pattern of gene findings involving the metabolic pathways for steroid and sex hormones that when combined with a drug like Finasteride that targets a key part of these pathways is almost certain to impact on how we metabolize these hormones more generally.
Problems can arise if we have a deletion in the relevant metabolic genes that normally offer a way to bypass a Finsteride obstruction. We can sail by on Finasteride with no problem if those genes are working fine in us.
Based on the deletion profile, Will predicted a set of likely results on Dutch tests. His prediction for PFS Dutch screens was broadly speaking right.
The PFS pattern is probably not going to hold true for PSSD or PAS for a few reasons.
Neither of these drugs directly impact on the metabolic pathways for these hormones the way Finasteride does. An indirect impact, however, is possible, especially with PAS, which does have some metabolic overlap with PFS.
Unlike Finasteride both PSSD and PAS affect women just as much as men and to some extent this is likely to lead to differences.
We can only be sure of what Dutch tests might tell us if we do them. Anyone getting a test kit, ideally needs to get a Dutch Complete Test – that includes dopamine metabolites.
There may be indirect routes to the same final result just as it looks like within the body there appears to be something that is leading PFS, PSSD and PAS folk to end up with a lot of clinical features in common.
It is worth nailing this down as these tests are simple and inexpensive and if the pattern doesn’t hold, it will steer any PSSD or PAS genome investigation in a different direction and perhaps offer hints on the best direction to follow.
There is another reason to move forward like this. In terms of sheer workload, no-one is going to be able to get through all the work single-handedly especially if it involves in the case of PSSD going back to genome scratch.
The great advantage for PSSD sufferers is that PFS and Will Powers have laid down a template for the kind of problem we are dealing with – a feedback loop disorder – even if the details for PSSD and PFS differ.
Confronting a genome without a focus like this is like looking out on the vastness of the universe. Finding something in a genome haystack is harder than finding a needle in a haystack – at least with the needle you have some idea what you are looking for.
It sounds great to hear that Will moved from genetic deletions to predicting Dutch test results. Deletions are a finite number – aren’t they? Not quite. We all have tens of thousands of deletions – so we still need a way to separate the chaff from the wheat and even then the work is likely to be painstaking.
Where Will’s strength and medical input more generally comes in lies in interpreting how we might move from some protein change or change in a metabolic pathway to a final clinical symptom.
The plan also is to apply with Dr Powers and others for a research grant to move this forward and establish that it is not just in his hands alone that promising results materialize. This may mean running higher powered and more expensive genome screens. If need be we will use RxISK Prize money to get this going.
Live With or Die From

Is it worth going ahead to get genome screens at this point using sequencing.com and gene.iobio to read the results the way Will has done?
There are yesses and nos to this.
Yes, because we are rapidly moving into an era where this can be done and more and more people will likely take it up, perhaps reading their own and family genomes to understand more about ourselves.
There is a need to remember here that genomes are likely to be like post-mortems – able to show what people can live with rather than die from.
Finasteride and other drug induced problems are different to the cancers, minor strokes and heart attacks we can live with and perhaps barely notice. They are more like a comet hitting the earth. These one off events offer a better chance of making a link to what has happened.
It’s likely that some people tinkering with genomes the way Will Powers did may come up with reasons why some of us have terrible problems stopping SSRIs or why SSRIs can increase blood alcohol levels for some or why anticonvulsants can weave their way into our nerves and close to become the problem we are trying to treat.
One of many Nos is that there are strict rules on holding genetic material. No one is allowed to hold other people’s genetic material unless it is a doctor or health system and then the holding is governed by strict rules aimed at protecting us from insurance companies finding our results and increasing our premium on the basis of our newly discovered risk profile.
In Will’s case, his work to date has been on his patients. Expanding this to overseas requests for input becomes a lot more complex if it also means he is left holding the gene baby.
If we can get to a point where we have a somewhat clear idea about what we are hunting for, stand a chance of finding it and have ways to return all screens to the individuals they came from rather than hold onto them, this will be a lot safer all round.
Having read the recent Rxisk post and, now, this one, I am left with a feeling that there is a message here which needs to be shared further than just between those of us who read it here. Is there any way that you could pinpoint the main points of interest which could be shared with members of our group, for example? My thoughts are that, if we are soon to be paying out from the Rxisk Research Fund, it may be a good time to share in the hope that more donations may come through
The suggested list would need to be in layman’s terms please, so that I can understand exactly what it is that I am trying to say to convince other people of a worthwhile use for their spare cash!
Mary
It’s very hard to boil it down into one message – between the two posts here on these issues and the two posts on rxisk the main message is laid out. The problem is it sounds different to the kind of message people are used to hearing and any attempt to have a brief pointed message may be even more confusing.
If I come up with a brainwave as to phrasing I will let you know. The bottom line I think is if someone who has lived in the midst of these issues for 20+ years figures it might be a good idea to invest the RxISK Prize money into what needs to happen that suggests there really is something here.
We would put all the money into research which might be interesting and could go on for decades without saving a life. The window that has opened up offers a chance to save lives starting maybe this year and there are a lot of lives being lost as it is or lives destroyed that decades of research might do nothing to prevent. Saving lives at the end of the day is more important that being absolutely sure of every fine detail.
D
I guess that one thing that would help would be the answer to this question :-
” is all that we’re hearing recently likely to help me, a sufferer of 16+ years, or are we pinning our hopes on something that could support future users of the mentioned drugs?
THAT, I guess, will be the first question that I anticipate being asked and am not sure how to respond to it!
Yes. My view is that there is something here that does more than offer an insight on what has gone wrong but also offers an opening to help at least some people recover probably completely.
Once some are clearly helped it will be impossible to ignore the problem and more research interest and funds will pour in.
D
Thanks – this is really comforting news for SO many who have felt totally helpless and hopeless for far too long.
I started thinking of ways to solve the DNA data privacy issue. It occurred to me that if we can’t have people shooting VCF files over gmail without moving operations to Kazakhstan, maybe we could make the data more abstract. Instead of looking at people’s genomes, is there an abstract way to just get a “show of hands” for variant lists of interest without seeing the bodies raising those hands. All that is shared is an integer, a count.
Searching around I found that this protocol already exists its called Beacon: https://www.ga4gh.org/product/beacon-api/
Its used by institutions but I thought perhaps there is no reason we couldn’t use the protocol.
How it might work specifically:
This proposal is for a small, simple system that lets the community ask and answer research questions like that at scale, while keeping every individual’s genome firmly on their own computer.
Someone in the community, I’m imagining it would be a researcher, curates lists of genetic variants worth investigating. They write up a simple text files containing those variants and post it on a suitable public platform, it might be a curated Github page, or any platform that can be curated. The file might be called something like “PSSD Variant list 14”.
Anyone who has their genetic data and wants to participate downloads the list and runs it through a small custom application on their own computer. The app loads their genome file, checks how many of the listed variants are present, and shows them a count: “You have 3 of these 12 variants.” That’s the moment the user decides whether to contribute. If they want to, they submit the number, just the number, “3”, to a public tally for that query. If they don’t, they close the app and nothing happens.
After enough people have submitted, someone tallies the responses and posts the aggregate finding: “Of 47 self-identified PSSD sufferers who ran Query 14, the average count was 1.8, with 31 people having at least one of the listed variants present.”
The assumption would be that self-selection pressure would ensure that mostly people who genuinely suspect they have the phenotype of interest will download the file and submit their count. You could further encourage this by providing clear instructions about the purpose of each list file and the phenotype it relates to on the website where the files are hosted.
No user information is shared, the researcher doesn’t see where the counts came from, they just see the raw tally.
Python has an existing library for parsing Variant Call Format (VCF) files and the application would be quite simple, just a GUI that lets users load up the list file, run the search and submit their count to the server. The only skills users would need would be the ability to download the application and enough of a clue to know what which one the VCF file is. I could probably build such an application, not that I’m any great programmer but it doesn’t need to do much.
Beacon V2 has some extra safety rails to prevent accidental leaks: query rate-limiting and minimum-N suppression. Query rate limiting prevents a leak by a Guess Who/Celebrity Heads kind of situation where you leak by posing too many overlapping variant queries. But it might not be needed in our use case as we would be convenience sampling a population of unknown size rather than a fixed institutional database, that is provided the variant query files were hosted on site accessible to the entire population, not just members of a Reddit or Facebook group. You can’t play Guess Who if you don’t know the number of faces on the board. Minimum-N suppression might still be needed but that is a no-brainer.
Thoughts on the idea? Useful? Useless? Still too legally grey? Too hard?
Peter
This is fabulous. The people damaged by meds from PSSD to lamotrigine induced problemds are among the most motivated people I know when it comes to something that looks like it could make a difference and especially if it could save lives.
I will be discussing options with several university departments in weeks to come and will run this by them to get their reactions.
Plus it is worth spreading the word around the PSSD groups and seeing if we can get some of these groups who have a lot of expertise to think things through.
Watch this space and will also keep you in the loop on other inputs
David
Good. Of course its just one possible method of abstracting the data for privacy based on Beacon, we might be able to come up with something better. It is also possible an existing platform could be repurposed for this sort of use, although so far I figure the moment you upload the VCF file to anything on the internet you then open up all the legal issues but then again, Gene.iobio is online and they apparently get around part of the legal issue by only streaming the parts of the genome that are being queried at any one moment so the whole genome is never stored “online” at once.
Peter
Thanks for this. We need to get some more online savvy folk to weigh in on this. we in this case means you – I’m out of my depth although you are putting things pretty clearly.
David
Yes, and some legal people too. Depending on the institutional involvement we might not even need to be as careful as I am proposing. If a private individual posts a variant list online and another private individual runs the list against their own genome on their own private computer and then posts online that they had matches for this or that variant, has any privacy law been violated? If its an instituition posting the variant lists and people are replying with their results to a practicing clinical researcher, that I think is more where the problem would be. But I think if you ask around between the tech savvy and legal savvy you’ll be able to find a way of going about it.
Just making it easier for people to run a variant checklist on their own computer might be helpful for people who can use a computer OK but don’t feel confident with tools like gene.iobio. It also prevents any confusion and people coming back saying “I looked and I have all of those genes!”. It might make it easier to roll out for controls as well, which we may still wind up needing.
Peter
This is fabulous. It’s also important. We don’t want expertise locked up – by expertise I mean sophisticated abilities to keep the rest of us engaging with matters that are important to us and having things left to a few illuminati to pontificate on – actually we do want that kind of expertise locked up.
There is a terrible fear that the ‘people’ will be irresponsible. This shows most clear when the system decides to tell the airheads what they can and can’t do – airheads being pregnant women – when in fact in my experience women who are pregnant or thinking about becoming pregnant are the group who do the most research and are the best at making finely judged benefit-risk calculations pertinent to them that I know.
I keep figuring we should put good registries in the hands of pregnant women detailing everything everyone takes in the year before, during the pregnancy and perhaps everything their child has for at least 2 years afterwards. This seems to me to be somewhat like the option you are opening up here.
We need to get as many people as we can looking at all sides of this
D
Yes it seems the right idea.
Some app running on the desktop/phone of the patient.
He would be in control of his data and also the app.
May be the code for data extraction/computation from the data
should be ”open” so that one can check there is no spying
on confidential information.
But on the server side, if you want to collect data for stats
you should check the consistency of data.
Imagine one pharma company wanting to spoil your data…
Thanks Vincent
Now we need someone who knows how to build something like this
D
Thinking about it. I see a technical challenge with that project. If I understand well the data collection/preprocessing should be done on the patients’ desktop with some
app we provide them with. In this case the data should have some standard format
so that the app can process them. The patient will not bother spending much time
entering data. So is there already some kind of standard format? Getting some fine big data for statistical treatment is often a pain.
As someone with almost no scientific education – I’ll risk a first stab at the kind of simple explanation Mary could use with her group – once it’s been corrected by you . If it’s salvageable at all.
What are we talking about – Metabolomics? Here’s a reasonably clear explanation from Wiki
‘Metabolomics is the comprehensive, large-scale study of metabolites—small molecule substrates, intermediates, and products—within cells, biofluids, or tissues. It gives us a SNAPSHOT OF A BIOLOGICAL SYSTEM’S METABOLIC STATE (the metabolome) at a specific time, allowing researchers to measure how diet, drugs, or diseases affect chemical processes’.
A new way of understanding how Post Finasteride Syndrome affects some people and not others
A US doctor, Will Powers, has made an intensive study of the genomes – genetic blueprints – of his patients with Post Finasteride Syndrome, on an impassioned mission to prevent even one more suicide. He has identified certain patterns (more than one pattern) in this infinitely complex mass of genetic data that differentiate those who have had life limiting reactions to finasteride and others who have not been troubled by the drug. These genomic patterns are associated with certain metabolic profiles- and this can be tested by examining the metabolites found in urine tests. Will’s hypotheses about the metabolites likely to be found in PFS sufferers’ urine have been largely accurate. He’s really onto something.
Why this feels like a possible breakthrough?
If we can understand how the bodies of those suffering extreme adverse reactions -including withdrawal – metabolise the chemicals they ingest – finasteride, SSRIs, isotretinoin – there is a chance that we might be able to reverse engineer this metabolic iatrogenesis.
For years we have been focusing on the science of receptors and chemical signalling to try and understand how psychotropic drugs work – and harm. But, to me it makes a lot more sense to try and understand how a substance we ingest is being metabolised within our bodies – and whether we can correct/adjust harmful metabolic processing.
(C+ A good attempt – quite well written, but must study harder).
Let’s see what Mary says. Here is another version.
A lot of people talk about research for conditions like PSSD but there is almost nothing happening. Most of mainstream medical research is good at keeping the studies going for decades without actually saving the lives that are being lost meanwhile. Maybe the research is focussed on the wrong thing.
Most research if focussed on finding a key to the lock that is a disorder. Will Powers has turned this around – PSSD and other conditions are more a case of a key getting stuck in the lock and we need to find ways to ungum the system. We can do this without understanding every little bit of the system we are dealing with. With a little bit of support – not just money – but both medical and lay folk looking at the problem in this light we may start saving lives this year.
D
I know ‘perfection is the enemy of good’ – as you have reminded me, a perfectionist, on occasion!- but I think this is a pretty perfect opening political statement.
In order to satisfy Mary though – a tough ask – either for use as a lay explanation or a fund raising communication – I don’t think you can leave it hanging there. Ideally imo it needs some uncomplicated info to support your promise, the reason to believe in marketing speak.
A few brief sentences on Will’s apparent breakthrough, applying these principles to PSSD, the research work/contribution Rxisk is planning – maybe a brief comment about how Metabolomics are used now – and how this way of seeing is a possible revolution.
But Mary is our judge…
We’re not on the same page here. It may be partly my fault for mentioning Metabolomics in a RxISK post. I had thought I was telling people that it was gobbeldygook or a version of Moliere;s skit on pretension – you mean Ive been talking prose all this this – golly gosh. But looks like i messed that one up.
Will may be wrong on a lot of the details so I’m not sure it will help to dive into the details – to act like pharma and use a catchy bit of biobabble – a phrase like it’s all got to do with lowered serotonin. The big picture is treatment has gummed up system, we’re not absolutely sure how but having this perspective opens up a lot of new treatment approaches that no one has been considering up till this.
My guess is we will be able to significantly help some people this year but not everyone and it will need getting a bunch of people onboard to understand how to tweak what works for some to enable us to help most and hopefully all
D
I watched Will’s interview with Robb and read some of his reddit threads (before you led me astray with ‘Metabaloney’- all the more confusing because it sounds relevant if pretensious). This one idea from Will – even if proven wrong-seems to shed a bit of light on the potential of an approach that otherwise feels like impenetrable genomic darkness and complexity to us layfolk.
‘But this was the first one I found, and is the most textbook. Anything that impacts your ability to metabolize androgens outside the usual scope, can negatively impact you. Anything that increases your androgenic synthesis above normal like ashwagandha, can plug you up with metabolites that you can’t clear properly. When this happens, your system is literally overloaded with androgens even though it may seem like you don’t have enough. It’s so crowded that the receptors can’t hear anything. And my current plan is to clear these out and then see what happens when I’ve unplugged the router and plug them back in.’
‘Aside from giving lab and genome findings across mostly all PFS patients that are finally consistent and reliably fucked up. That’s never happened before. It seems nearly every single PFS patient is built like this and when they aren’t, I can still find the “why” in the genome as there will be some other “almost” catastrophic metabolism problem that when fin is added to the mix, results in the true catastrophe.’
I clocked your satirical tone re ‘Metabolomics’. It reminded me, not of Moliere, but of that classic Maureen Lipman ad for BT. when her grandson, Anthony, tells her he’s failed all his exams except pottery and sociology. ‘ You’ve failed? You’ve got an ‘ology’.
You’ve picked out a great quote. Now the trick is to find what happens in PSSD. RxISK has lots of PSSD – PFS like reports linked to Ashwagandha – I assumed there was a serotonin reuptake inhibiting link with A – but maybe its both SSRI and Fin like
D
A squittering of news out of the cave
Finasteride and Dutasteride – updated safety warnings for psychiatric side effects and sexual dysfunction
The MHRA has reviewed the evidence for finasteride and dutasteride and the risk of suicidal thoughts and behaviours and has recommended further measures to minimise this risk.
https://www.gov.uk/drug-safety-update/finasteride-and-dutasteride-updated-safety-warnings-for-psychiatric-side-effects-and-sexual-dysfunction
Dr Alison Cave, MHRA chief safety officer, said: “The MHRA has taken significant action to raise awareness of the risks of sexual dysfunction, depression and suicidal thoughts associated with finasteride, including issuing a Drug Safety Update and introducing patient alert cards in 2024.
Following an additional detailed review of the evidence, we have now strengthened product information for both finasteride 1mg and dutasteride to provide clearer guidance on these potential risks and to support informed discussions between healthcare professionals and patients.
“Patient safety is our top priority. We expect prescribers to discuss the relevant safety information with patients so they can make informed decisions about their treatment, and we continue to encourage patients and healthcare professionals to report suspected side effects through the Yellow Card scheme.”