This is the final post in the Bruce Willis series – see Osama, Obama and Reckless. It’s the point behind the series. And it comes on the 28th anniversary of the original event.
Train Tracks
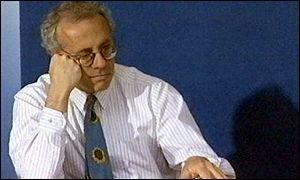
Its 1991. Two trains are heading toward each other on the same piece of track. One has a shiny badge that was new for trainspotters – Evidence Based Medicine (EBM). It had been assembled in part in Canada’s McMaster University by David Sackett and Gordon Guyatt among others and in the UK by Iain Chalmers and others. Richard Smith (photo), then the editor of the British Medical Journal (BMJ), was an enthusiast for this new marvel.
In 1980s, pharmaceutical companies were perceived like Sauron in Mordor as growing in strength. Organisations like No Free Lunch appeared. Physicians were hearing they should be wary of the Wooden Horse sitting outside the gates of medicine.
A medicine under siege breathed a sigh of relief when EBM arrived in town and seemed to solve the problem. Doctors were given weapons to fight pharmaceutical companies with. The vampires with their sales and marketing tactics would shrink back faced with the crucifixes and garlic of evidence held up in front of them.
It wasn’t put like that. More a case of in the face of the obvious, the lion would voluntarily lie down with the lamb. Bash industry? Not us. Just scientists here.
In 1984, the US pharmaceutical industry generated $24 Billion of revenue per year. A decade later, a single drug alone could generate $10 billion per year. The pharmaceutical industry had found a way to make the powder in their capsules worth more than its weight in gold.
Prozac which launched in 1988 was one of the exemplars of the other train rolling down the track toward the shiny new EB Medicine. If you wanted a decent drug – something that would be at least as strong as the pills we already had, and ideally safer, or maybe able to treat something we had not been able to treat before, this wasn’t that pill. It was less effective than already available and cheaper pills and there were good grounds from the get-go to think it and anything related to it might be hazardous.
Should have been no contest. EBM should have rolled right over Prozac.
Especially as Prozac was almost derailed before it had fully picked up speed. Pesky patients went and got themselves suicidal on it. An article appeared in the American Journal of Psychiatry in 1990 outlining 6 cases of people with suicidality that had emerged on treatment. The paper came from Harvard. One of the authors, Jonathan Cole, was just about as distinguished and at the same time sensible as anyone could be. Thousands of patients lined up across the US claiming they had become suicidal on the drug.
The company had three responses – these are anecdotes, its the disease not the drug and it’s all just being rustled up by the Church of Scientology.
September 1991
The trains met in September 1991 – thanks to Richard Smith.
Central to Lilly’s efforts to defend Prozac was a meta-analysis (a new term then – part of a lexicon EBM was introducing) of the clinical trials of Prozac, looking at rates of suicidal events on the drug. Very few journals had seen data handled like this before.
Whether the novelty of an article like this meant it didn’t work for the first journal it was sent to, or the very obvious increase in risk on Prozac, it was turned down and ended up with the BMJ.
The BMJ reviewers demurred at the proposed title which suggested Prozac reduced the risks of suicide. The claim was made on the basis that Hamilton Rating Scale scores fell on the drug but ignoring the fact there were more suicidal events on Prozac.
Looking at the paper later published in the BMJ, with Charles Beasley as first author – HERE – in placebo controlled trials there were 5 suicidal events in 1398 patients taking Prozac and 1 in 645 taking placebo. More on Prozac – but it was not statistically significant – which everyone was told meant there were no suicidal events on Prozac in other words. Move on – nothing here to look at
However looking at the small print the placebo suicidal event happened in the washout period so there were in fact no events on placebo and the risks on Prozac were statistically infinitely greater than the risk of placebo. It doesn’t look like the reviewer can have looked at the small print.
Richard Smith (for whatever reason) certainly didn’t look closely. He had in his hands a major company signing up to embrace the EBM he was promoting at every turn. If all companies ended up following (being forced to) this example, the world would spin more happily on its axis from here on.
Oh Happy Band of Brothers, you will be able to tell your children that you were here with me and the BMJ on St Candida’s Day.
The article came out in the September 20 1991 edition of the BMJ. coinciding with FDA hearings on Prozac and suicide. Given the patient groups springing up all over the place in the wake of Prozac’s launch, with hundreds of reports to FDA of suicides or suicidal events, FDA was forced into a public hearing.
At the hearing, company people and company experts (people), notably Charlie Nemeroff, were brandishing the Beasley paper – look it says here in the BMJ there is no risk from Prozac. Which are you going to believe the anecdotes or the science. The plural of anecdote is not data.
The Little People
The FDA committee recognised the compelling testimonies from the little people whose husbands or children or parents had blown their brains out or who had died in other horrific ways. A few weeks after starting Prozac, Joseph Wesbecker, who featured in the news last week, two years and one week before, had killed 12 at the Standard Gravure plant in Kentucky, before blowing his own brains out.
But their hands were tied. There was no basis in the science to say Prozac had caused this.
It wouldn’t even be a good idea to warn about a possible risk because that might put people off seeking treatment and the benefits they could get from Prozac.
Prozac sales had been falling. They recovered after the FDA hearing.
Become Invisible
The effect on medicine and the rest of us was far-reaching. Journals like the BMJ stopped taking articles like the Teicher and Cole paper outlining 6 convincing cases of suicidality induced by Prozac. FDA had just ruled this is not evidence. Journals might be sued for publishing them – besides which they made no money from them.
A premium was put on ghostwritten clinical trials with no access to the trial data and even more on meta-analyses – companies paid vast fortunes for reprints of these making BMJ and other journals profitable indeed wealthy if they wanted.
Richard Smith could have demanded access to the raw data in exchange for publication in BMJ. He didn’t.
But he got a sales-force for EBM. Companies now encouraged doctors to prescribe according to the evidence and to stop paying heed to the appearances of people in front of them or to what they say. Everyone knows that patients and doctors can’t work out what drugs do – only controlled trials can do that.
Patients became invisible – just as doctors and everyone else in healthcare did too. If practice is going to be scientific it has to be according to the evidence, embodied in guidelines which dictate what drug is given in what sequence.
If this is the case of course who needs high cost prescribers. We can have nurses, pharmacists, AMPs or whoever – told keep to the evidence based guidelines or you get fired.
And we can replace everyone with locums. Who needs relationships if whoever is there sticks to the “Evidence”.
As a result it now takes 30 years to get recognition of the common problems on patent drugs cause.
Gallileo
Clinical Science is incompatible with a top-down-archy. Hierarchy is not the right word here – as hieros means sacred or moral. Its Gallilean or nothing.
The first task is to work out whether the drug this person took has caused the effect they now mention or not. Having reviewed all the evidence if we both think it has and this is at odds with what the Evidence Base appears to suggest, the second scientific task is to explain the discrepancy. In the case of the SSRIs and suicide, there was no discrepancy once we got to see the clinical trial data. If it is to have any credibility, EBM has to be Data Based Medicine.
Waving or Drowning
Well done Richard on a Bruce Willis award.


‘Evidence Based’ Medicine
Antidepressants linked to murders and murderous thoughts
https://www.telegraph.co.uk/science/2017/07/25/antidepressants-linked-murders-murderous-thoughts/
Sarah Knapton, Science Editor
26 July 2017
“But it’s happened just too frequently with this class of drug to make it random. It’s obviously related to the drug but we don’t know exactly why.”
The role of the drugs was not explored in court
“Although it makes the whole process a bit more complicated, I think that is going to become necessary in the future.”
The Batman Killer –
a prescription for murder?
Shelley Jofre
https://www.bbc.co.uk/news/resources/idt-sh/aurora_shooting
Where is the evidence; Sertraline did not cause James to have a complete personality change
The cost of vaccinating a single child went up by 68 times between 2001 and 2014
https://www.bmj.com/content/366/bmj.l5576/rr-4
and no one was hurt! It was discovered that you could inject a child with 10,000 vaccines in one go, and it couldn’t possibly cause any harm. British health officials still apparently maintain this! It is all science and perfectly evidence based.
https://www.ageofautism.com/2019/08/review-of-the-united-kingdom-national-health-service-webpage-why-vaccination-is-safe-and-important-m.html
Seems EBM more often represents Effectively Biased Medicine, unbeknownst to countless martyrs who die early, avoidable deaths due to their apparently dangerous belief: “In doctors and medicine we trust.”
Unlike St. Candida, their remains are not enshrined nor blessed by the Pope. Instead these martyrs lie in commonplace graves that are sometimes visited by bewildered, grieving family members who will never learn what precipitated such traumatic sudden deaths.
It remains difficult for me to fully comprehend that the runaway train fueling Prozac’s approval and blockbuster sales was set in motion years before my now-dead teen was even conceived.
Can’t help but wonder what current drugs are being promoted today based on EBM that will later precipitate the demise of babies who are presently safeguarded in their happy mothers’ wombs.
Very Sorry I just cant remember who it was who was flagging up concerns about drug shortages a while ago – there’s a whole list been published now
Shortage Notice: Fluoxetine 10mg, 30mg and 40mg capsules
September 20, 2019
Morningside and Advanz, the manufacturers of Fluoxetine 10mg, 30mg and 40mg capsules, are currently experiencing temporary disruptions.
Please see a table below which summarises the overall fluoxetine availability:
Supplies are available from specialist importers on an ‘unlicensed’ basis. Ensure that where a prescriber wishes you to dispense an import, prescriptions are annotated ‘Special Order’ and are endorsed as follows:
Quantity dispensed
Pack size
Price per pack less any discount/rebate
Manufacturer/importer MHRA license number
Batch number
Specials procurement fee endorsement of ‘SP‘
All prescriptions for unlicensed medicines should be placed in the red separators for the end of month submission.
Click here to see the full communication from Department of Health and Social Care. Google ‘shortages of drug supplies.’
See our factsheet for further guidance on endorsing unlicensed specials and imports.Patients must be ‘urgently’ referred back to mental health specialists if drug shortages hit, SPS warns
17 JUL 2019 11:00
Patients who take medication used to treat depression should be “urgently” referred back to a mental health specialist if their supply runs out, the Specialist Pharmacy Service has warned.
Richard Smith: Stephen Lock, one of the best BMJ editors, is 90
April 8, 2019
Richard Smith 2 “Editors of The BMJ are alternating fools and bastards,”
said Stephen Lock, my predecessor as editor of The BMJ, who has a gift for memorable axioms.
Stephen is clear that his predecessor Martin Ware, an old Etonian, was a fool; indeed, Stephen thinks that old Etonians are the source of many of Britain’s problems, a sentiment that seems exactly right looking at their role in the Brexit farrago. Ware’s predecessor, Hugh Clegg, was proud of being a bastard and frightened even Stephen. ………I’ve declared myself to be a fool, along the lines romantically of Lear’s fool, ……Stephen has no doubt that he is a bastard.
Stephen also taught me about research fraud.
He became concerned about it in the 80s when most scientific authorities thought it unimportant—because it hardly ever happened, never harmed anybody, and didn’t matter because science is self-correcting (all of which are wrong). He managed to convince the Royal College of Physicians to produce a report on the subject, which he wrote. He didn’t succeed in getting the scientific authorities to take the problem seriously, and everybody, including me, thought him a little crazy and obsessed. But it was us who were badly wrong. Stephen wasn’t surprised that the authorities were so lethargic, pointing out that the Royal Society still had slaves ten years after slavery was abolished.
Another subject where Stephen was way ahead of others was research into editorial processes—or “journalology,” as he christened it. Scientists who should demand evidence for all that they do abandoned the concept when it came to the processes of publishing science. Peer review, which is central to science and still, I argue, faith rather than evidence based, was largely unexamined until Stephen began to research it. He discovered, for example, that most of the 90% or so studies rejected by The BMJ were published elsewhere usually unchanged in response to the reviewers’ comments. His book A Difficult Balance: Editorial Peer Review in Medicine is one of the best things written on peer review.
Stephen raised the scientific standards of The BMJ, particularly by introducing statistical review, which was unusual at the time, and “the hanging committee” a group of researchers and clinicians who together with editors reviewed the science and judged what would interest readers. (The committee was named by Stephen after the committee of the Royal Academy that decided which pictures submitted for the annual show should be hung). But Stephen also recognised that many readers of The BMJ were not much interested in the research and so he introduced features like ABCs and Minerva, which made the journal much more useful and accessible to doctors.
delusional bastards haven’t all been to Eton.
I fear Smith was more like Puck getting in a tangle than the Fool in Lear: but unfortunately it was Puck in a tragedy and he couldn’t sort it out.
He was offered a way out of it. All sorts of internal documents that made it very clear what was going on plus an article putting them all in context but he declined to publish. And sabotaged several other efforts to let a wider world know about what was going on.
D
David
I am sure that’s true too. I was thinking about his flippancy over the years over a host of things – I have long ago lost track.
John
More hot air or …?
DepartmentsWorldwideHow government worksGet involvedConsultationsStatisticsNews and communications
The United Kingdom is leaving the European Union on 31 October 2019.
Get ready for Brexit
Hide message (eh?)
Home Health and social carePublic health Health improvement Drug misuse and dependency ( why in the same actegory as misuse?)
Press release
Dependence on prescription medicines linked to deprivation
PHE has published the first-ever evidence review of dependence and withdrawal problems associated with 5 commonly prescribed classes of medicines in England.
Published 10 September 2019
From:
Public Health England
Bottles of prescription medication
The Prescribed medicines review assesses the scale and distribution of prescribed medicines – and makes recommendations for better monitoring, treatment and support for patients.
It uses available prescriptions data, a literature review and reports of patients’ experiences. (Available?)
A total of 5 classes of medicines were included in the review:
benzodiazepines (mainly prescribed for anxiety and insomnia)
Z-drugs (insomnia)
gabapentinoids (neuropathic pain)
opioid pain medications (for chronic non-cancer pain such as low back pain and injury-related and degenerative joint disease)
antidepressants (depression)
The main findings include:
1 in 4 adults had been prescribed at least one of these classes of medicines in the year ending March 2018
in March 2018 half of those receiving a prescription (of these classes of medicine) had been continuously prescribed for at least the previous 12 months. Between 22% and 32% (depending on the medicine class) had received a prescription for at least the previous 3 years
long-term prescribing of opioid pain medicines and benzodiazepines is falling but still occurs frequently – which is not in line with the guidelines or evidence on effectiveness
Trends in prescribing include:
the number of prescriptions for antidepressants and gabapentinoids are rising
following years of increase prior to 2016, prescriptions for opioid pain medicines and z-drugs are now falling
prescriptions for benzodiazepines continue to fall, as they were prior to 2016
women and older adults (particularly over-75s) are prescribed to at the highest rates
Links to deprivation include:
prescribing rates and duration of prescription are higher in some of the most deprived areas of England
a similar pattern is also seen for the number of medicines co-prescribed (for example, at least 2 of the drugs)
for opioids and gabapentinoids, the prescribing rate in the most deprived quintile was 1.6 times the rate in the least deprived quintile
the co-prescribing rate in the most deprived quintile was 1.4 times higher than in the least deprived quintile (30% compared to 21%)
Opioids for chronic non-cancer pain are known to be ineffective for most people when used long-term (over 3 months), while benzodiazepines are not recommended to be used for longer than 28 days. The review identified that when first used these medicines are prescribed for short term use. However, some patients do still end up being prescribed these medicines for longer periods. (and whaty’s been done about that?)
Long-term prescribing is likely to result in dependence or withdrawal problems, but it is not possible to put an exact figure on the prevalence of dependence and withdrawal from current data.
People who have been on these drugs for longer time periods should not stop taking their medication suddenly. If they are concerned, they should seek the support of their GP.
People who had experienced problems from prescription medicines also reported that they felt uninformed before they started them, and unsupported when they experienced problems.
The drugs in this review are vitally important (when prescribed properly) for the health and wellbeing of many patients. It is important that doctors follow the clinical guidelines and do not put inappropriate limits on prescribing that could cause patients’ harm or drive them to seek drugs from illicit sources.(they are still thinking – illegal drug taking – how many really do know where to go for illicit drugs?)
The review makes a number of recommendations focusing on education and treatment, including:
giving NHS commissioners and doctors better access to data, (Honestly – when will the be given this?)improving insight of prescribing behaviour in their local area and enabling GPs to follow best practice (‘best’ – meaning?)
updating clinical guidance for medicines which can cause problems with dependence and withdrawal, and improving training for clinicians to ensure their prescribing adheres to best practice
to develop new clinical guidance on the safe management of dependence and withdrawal problems
giving better information to patients about the benefits and risks with these medicines
doctors should have clear discussions with patients – and where appropriate offer alternatives, such as social prescribing
commissioners ensure appropriate support is available locally for patients experiencing problems (where are they?)
a national helpline for patients to be set up
ensuring high-quality research around dependence and withdrawal is undertaken
PHE has also published a detailed geographical breakdown by clinical commissioning groups of prescribing rates for 2017 to 2018 and the proportion of people that had been receiving a prescription for at least 12 months prior to March 2018.
Rosanna O’Connor, Director of Alcohol, Drugs, Tobacco and Justice at PHE said:
We know that GPs in some of the more deprived areas are under great pressure but, as this review highlights, more needs to be done to educate and support patients, (patient blaming)as well as looking closely at prescribing practice, and what alternative treatments are available locally. (where?)
While the scale and nature of opioid prescribing does not reflect the so-called crisis in North America, the NHS needs to take action now to protect patients. (How long do they need?)
Our recommendations have been developed with expert medical royal colleges, the NHS and patients that have experienced long-term problems. The practical package of measures will make a difference to help prevent problems arising and support those that are struggling on these medications.
Professor Paul Cosford, Emeritus Medical Director at PHE said:
These medicines have many vital clinical uses and can make a big difference to people’s quality of life and for some their long-term use is clinically necessary, particularly antidepressants, which can take longer to have their full effect.
This report shows that while the vast majority of new prescriptions for these medicines are for short term use, within clinical guidelines, it also highlights significant numbers have been taking these medicines for a long time. It is vital that clinical guidelines for prescribing are followed and regular reviews with patients take place to address this.
We also know how difficult it is for some people to come off these medicines and more research is needed for us to understand better how we help people to stop using them when they are no longer clinically helpful. (Plenty of research already there Paul C – check out Rxisk for a start)
Keith Ridge, Chief Pharmaceutical Officer at NHS England, said:
As PHE rightly say, these medicines have many vital clinical uses and can make a big difference to people’s quality of life and for some their long-term use is clinically necessary, particularly antidepressants, which can take longer to have their full effect.
But for many patients they may not be the best option – with talking therapies and social prescribing often more appropriate. (repeat after me – endlessly ..other options are more appropriate – where are they Keith R?)
Arabella Tresilian, a patient who has experienced problems associated with withdrawal, said:
I was on and off anti-depressants for over twenty years, juggling work and family life at the same time. I really struggled to come off them and in 2015 I was diagnosed with post-traumatic stress disorder and chronic fatigue. Day to day activities became overwhelming and I quickly began to feel isolated.
I was very lucky that my doctor’s surgery (presumably the one which had been precribing for over 20years)offered social prescribing which made all the difference. They referred me to a local choir which helped me with my recovery and gave me back my confidence.
I know first-hand that dependence and withdrawal from prescription medicines can be extremely difficult to cope with. It is reassuring that this review recognises that more needs to be done and I am hopeful that social prescribing will now be offered more widely.
Background
The review analysed available NHS prescriptions data from community pharmacies from April 2015 to March 2018 on 5 classes of prescribed medicines:
antidepressants
opioids
gabapentinoids (gabapentin and pregabalin)
benzodiazepines
z-drugs
It also included a rapid evidence assessment of literature on the harms caused by dependence or withdrawal, risk factors, treatment and prevention interventions and the support patients receive.
An expert reference group, made up of a broad range of specialists and experts by experience, was recruited to provide advice and support for the project.
The Prescribed Medicines Review (PMR) brought together the best available evidence, following PRISMA guidelines, on:
prevalence and prescribing patterns in adults
the nature and risk factors of dependence and withdrawal symptoms associated with prescribed medicines among some adults who take these medicines
effective prevention and treatment of dependence and withdrawal for each drug category Supportive statements
Dr Norma O’Flynn, Chief Operating Officer of the National Guideline Centre at the Royal College of Physicians said:
We’re pleased to be able to support the work of PHE on their prescriptions medicines review by conducting systematic reviews of the research evidence.
The reviews and report recommendations are important steps in promoting a focus on managing prescription and withdrawal and highlighting areas where more research is required to inform practice.
Professor John Read from University of East London, speaking on behalf of the British Psychological Society’s representative on the PHE review’s Expert Reference Group said:
We thank Public Health England for all its work on this hugely important report.
We especially welcome the thorough research review documenting the alarming numbers of people experiencing withdrawal effects from prescribed medicines, and the recommendations for urgently needed services and a phone line to support people struggling to come off these drugs, including antidepressants.
We also value the emphasis placed on increasing accessibility to talking therapies for the problems that the drugs are currently prescribed for.
Public Health England press office
Wellington House
133-155 Waterloo Road
London
SE1 8UG
Email
phe-pressoffice@phe.gov.uk
Centre receives funding for its Early Years Programme
23rd August 2019 By: Michelle Cunliffe
The Department of Health and Social Care announced an investment of £3.3 million in 23 local community projects across England – one of which is the Anna Freud Centre’s Early Years Programme.
The funding will come from the Health and Wellbeing Fund to help expand and evaluate already successful, innovative projects that adopt community and person-centred approaches to improving the mental health of children and young people aged 0-25 years.
The three-year project enables the Centre to expand our existing early years work in the boroughs of Camden and Wandsworth to create a fully integrated infant mental health pathway. This pathway provides a continuum of early years provision from universal to targeted to specialist services and a shared language of understanding and intervening with families and young children across all front-line early years’ professionals. Across Camden and Wandsworth, this will include workforce training and supervision, direct delivery of therapeutic interventions such as parent-infant therapy and toddler groups, as well as specialist consultation for social workers when infants are in families on the edge of care.
NHS Digital’s children and young people’s mental health survey reported that 5.5% of 2-4 years olds in England were identified with a mental health disorder in 2017.
In recent years there has been an emerging consensus around the importance of the first critical 1001 days for long term child development, with a focus on preventing infant mental health problems to help children get the best start in life.
Dr Camilla Rosan, Head of the Early Years Programme at the Anna Freud Centre, says: “The Anna Freud Centre is delighted to have been awarded this grant, and with the funding we will be able to engage a wider breadth of the most vulnerable families who currently fall through the gaps between health and social care and are not engaging in infant mental health services.
“All children deserve the best start in life. We know an infant’s earliest experiences shape their brain and can have an impact on their mental health into adulthood. Infanthood is a sensitive period during which babies’ socio-emotional and cognitive development is adversely impacted by the stressful life events that this programme is trying to target, including couple conflict or domestic abuse, worklessness, unstable housing and mental health difficulties.
“By supporting the parent-child relationship at this crucial early stage we can have a positive impact on mental health outcomes for all families.”
The projects will be fully funded through the scheme in their first year and the Anna Freud Centre has been awarded £139,483. Additional joint funding from Camden and Wandsworth Local Authorities has been agreed for the final two years.
Anna Freud Centre
Kantor Centre of Excellence
4-8 Rodney Street
London N1 9JH
Yet more funds for the Anna Freud-Kantor Centre of Excellence There are so many other small groups surviving on peanuts and goodwill of unpaid workers – is this the way to go ? Projects being influenced and funded by the personal values of billionaires What is not mentioned is that very young children are being scanned for brain differences at UCL where Peter Fonagay , colleague of Kantor ,and colleagues work on child development – it’s not all as innocent as it seems.
Two, Word-Smiths..
Richard Smith: Should scientific fraud be a criminal offence?
December 9, 2013
AntiDepAware • 6 years ago
The “chemical imbalance” fraud has made millions and cost lives. It can’t be regarded as anything other than criminal.
The No.1 Ladies Detective Agency author gets his material from somewhere,
“This is but one more instance where the bare-naked emperor of the academic and publishing communities is strutting about.”
https://blogs.bmj.com/bmj/2013/12/09/richard-smith-should-scientific-fraud-be-a-criminal-offence/
Study 329: BMJ Transparency
https://davidhealy.org/study-329-bmj-transparency/
annie says:
November 6, 2015 at 4:43 am
Good Work, Leonie, No. 1 Ladies Detective Agency
“EBM” – McCall the Cops …
There should also be information including warnings about potential ‘adverse effects’ as with prescriptions given to anybody thinking of therapy. The NHS cannot enough of what people want (or mainly only provide low quality time limited sessions) so one option is low fee or private therapy , the low fee is mainly provided by students in training with one of the many therapy organisations. It might be expected that providing the students with training would be free or that the institution would pay a client for allowing a student to practice on them ,but when feeling vulnerable few question tthe only thing they can afford. However none of the organisations or individuals running them them are regulated in the way other professions are. If a client is dissatified or the therapist behaves unethically a complaint can be heard by the organisation and ‘therapist can be struck of their register – but still continue to practice outside any registration- incredibly anybody can set themselves up as a therapist perfectly legally. The well being and mental health industry is one of the fastest expanding businesses in UK and elsewhere. eg It is perfectly aceptable in their view to charge from £50-£90 per session. Online ‘therapy’ is a huge business with little outlay and no obligatory qualifications. The issue of no regulatory protection has been running for decades but internecine quarrels amongs the organisations has helped to avoid it happening.
As for social prescribing we need to check out why one of the richest Russian oligarchs living in UK is providing billions to provide projects around the country inlcluding part funding the Kantor Center of Excellence-Anna Freud Centre in London. and projects set up with UK govnmt (Kantor sits on a peace cttee with Tony Blair) -led by Peter Fonagay Head of Anna freud Centre
Where some of the cash comes from:-Acron – (The Kantor center is in a prime location in London where previously ‘poor’ people could afford to live. Check out the overblown Kantor Building)
About ACRON (also a company producing fertiliser)
Building wealth for investors with real estate assets is our mission since 1981.including in UK and maybe a deal over the Kantor center?
Safe, solid, transparent!
Founded in 1981, ACRON is headquartered in Switzerland and the United States with business entities in Luxembourg, Germany, and Brazil.
ACRON focuses on real estate investments for wealthy private clients.
ACRON offers the advantage of first-class assets, trophy properties and prime projects in the world’s safe havens.
The oligarchs list is copied from the Forbes magazine
In 2017, Forbes estimated Kantor’s net worth at $3.1 billion,
Kantor is a generous benefactor and philanthropist to many causes
Anna Freud Centre
Kantor is a trustee and Life President of the Anna Freud Centre (London, UK).[22][23] He is actively supporting the organization in its groundbreaking work for children, young people and their families who are experiencing mental health issues. Kantor is helping to build the new Kantor Centre of Excellence in London’s King’s Cross as an extension of the Anna Freud Centre. The project will bring together the very best in science, education and mental health to support vulnerable families. At the heart of the project is a school for 48 children with emotional problems who have been excluded from mainstream education and require specialist and dedicated support.
Honors and awards
Kantor received the following government awards: Order of Friendship (Russia, 1998), Officer’s Cross of the Order of Merit (Poland, 2005), Order of Prince Yaroslav the Wise (Ukraine, 2006), Order of Leopold (Belgium, 2009), Chevalier of the National Order of the Legion of Honour (France, 2012), the Knight Grand Cross of the Order of Merit of the Italian Republic (Italy, 2013), Grand Cross with honours of the State Order for Merit (Romania, 2014), Officer of the National Order of the Legion of Honour (France, 2014, presented in 2015) and The Order of Honour (Russia, 2016).
In addition, he received an honorary doctorate from Tel-Aviv University (2004);[33] the Medal of Merit for Medal “Deserved for Tolerance” by the Ecumenical Foundation Tolerance (2011); and the European Jewish Leadership Award (2012).
Kantor has been recognized for seven consecutive years as one of the ’50 Most Influential Jews in the World’.[34]
See also
European Jewish Congress
World Jewish Congress
European Council on Tolerance and Reconciliation
International Luxembourg Forum on Preventing Nuclear Catastrophe
European Jewish Fund
World Holocaust Forum
Museum of Avant-Garde Mastery
References
Moshe Kantor to head WJC Policy Council
Ynetnews, May 08, 2013
Forbes. The World’s Billionaires
Forbes. The World’s Billionaires. | Forbes.com
Times, The Sunday (May 12, 2019). “Rich List 2019: profiles 53–100, featuring Mike Ashley and Bernie Ecclestone”. ISSN 0140-0460. Retrieved August 6, 2019.
/ Acron Group’s Fertiliser Output Up Increases 16% in 2017
Forbes. The World’s Billionaires
Forbes. The World’s Billionaires. | Forbes.com
“Honorary Citizens of Veliky Novgorod at the City Administration website – Viatcheslav Kantor – 08.09.1953”. Archived from the original on April 10, 2017. Retrieved April 10, 2017.
“Report to Congress Pursuant to Section 241 of the Countering America’s Adversaries Through Sanctions Act of 2017 Regarding Senior Foreign Political Figures and Oligarchs in the Russian Federation and Russian Parastatal Entities” (PDF). January 29, 2018.
“Viatcheslav Moshe Kantor – biography”. Retrieved October 20, 2013.
‘Manifesto on Secure Tolerance’, by Viatcheslav Moshe Kantor
Our Mission – European Jewish Congress
‘Holocaust didn’t erase Jewish life’. Center for study of contemporary European Jewry opens at TAU. The Jerusalem Post, May 10, 2010.
New Executive Committee of World Jewish Congress, Wed, 05 Jun 2013.
“EJC President Moshe Kantor re-elected as Chairman of World Jewish Congress’ Policy Council”. Archived from the original on August 26, 2017. Retrieved April 28, 2017.
“Vice Presidents”. Jewish Leadership Council. Retrieved September 2, 2019.
Tony Blair appointed as head of European body fighting antisemitism | The Guardian, June 4, 2015
ECTR Announces Research Grants and Kantor Prize for Secure Tolerance
A series of interviews with experts of the Luxembourg Forum, aired by Russia Today TV channel, July 2009
https://sacc-ejc.org/ Security and Crisis Centre by EJC
Anna Freud Centre
Trustees of Anna Freud Centre
Kantor King Solomon High School
King Solomon school changes name in Jewish leader’s honour / Jewish News — November 11, 2016
Royal Opera House Boards and Committees
Malovishersky psychoneurological nursing home to be re-opened after repair / Komsomolskaya Pravda — St. Petersburg, February 10, 2015
The Holocaust History Museum Donors
Museum of Avant-Garde Mastery
Forbes, January 26, 2014, “You cannot buy what you really want without paying too much”
President of the Museum of Avant-Garde Mastery Viatcheslav Kantor elected Honorary Member of the Russian Academy of Arts
Bashinform, September 17, 2018, “The Winner of the Vladimir Spivakov Contest Will Get a Violin for $140,000”
Tel Aviv University Webflash – May 2004
“The Jerusalem Post’s 50 most influential Jews”. The Jerusalem Post. Retrieved May 21, 2015.
External links
Viatcheslav Moshe Kantor (website)
European Jewish Congress
International Luxembourg Forum on Preventing Nuclear Catastrophe
European Jewish Fund
Security and Crisis Centre by EJC
Kantor Center on the Study of Contemporary European Jewry
World Holocaust Forum Foundation
An interview to the IBA TV on YouTube
National Institute of Corporate Reform
Authority control Edit this at Wikidata
LCCN: no2015058821VIAF: 315944482WorldCat Identities (via VIAF): 315944482
Categories: 1953 birthsLiving peopleMuseum foundersJewish anti-racism activistsRussian JewsRussian billionairesRussian businesspeopleOfficiers of the Légion d’honneurChevaliers of the Légion d’honneurKnights Grand Cross of the Order of Merit of the Italian RepublicRecipients of the Order of FriendshipRecipients of the Order of Prince Yaroslav the WiseOfficers of the Order of Merit of the Republic of PolandRecipients of the Order of Honour (Russia)Recipients of the Order of Merit of the Italian Republic
Could it be that philanthropy is providing tax advantages to not only pharmaceutical comanies – but importantly are effecting health provision on a massive scale.?
Bobby Fiddaman shared a link.
Visual storyteller · 1 hr
…
Appleby shared with his 19,000+ followers a tweet that made assertions that people who ask questions that are, seemingly, difficult for him to answer are “a dangerous cult”.
fiddaman.blogspot.com
Suicide Expert Embroilled in Twitter Controversy
Appleby, who has been repeatedly asked by drug safety advocates on…
In thebmj
Response
Re: Gender dysphoria in children: puberty blockers study draws further criticism
It is surprising to see that BMJ has commissioned journalists to be writing for a world leading medical journal on the topic of research into hormone treatment for young people with gender dysphoria. Such a topic requires medical research and research ethics expertise. It is hard to say why journalists are the appropriate people to write such a paper and a quick google search shows that some of the sources they cite clearly have an established ideological position.
Dr Merle Spriggs
Senior Research Fellow in Bioethics
University of Melbourne
Melbourne, Australia