Big Bias (video here) may be the most important lecture I have ever given. Its not easy. The bottom line is that Clinical Trials don’t work. For everyone working in health (medical Catholics), this is a bit like saying the Pope is not infallible. We have a great problem with this, partly because our response is – If not the Pope, then who? – the idea that no-one is infallible is beyond difficult.
The BB Slides are here and the text to go with these slides is below
This talk appeared as an article in the BMJ six weeks ago – Clinical Judgment, not Algorithms are key to Patient Safety – written a code called English. The talk strips away the code.
2). In this X-Ray you see my broken shoulder. I slipped in the shower on a Friday morning. It was fortunate I didn’t come to more grief. My shoulder was operated on later that day and I was back in work on Monday. This was good for me, for the hospital I work in who didn’t have to pay for a locum, for the patients who didn’t have to see anyone else, for my family and friends. Healthcare like this could be provided for free – it pays for itself.
3). A few weeks later I got a letter, which shows what is bankrupting healthcare. A letter like this is sent to everyone over a certain age who’s had a fracture treated in any UK hospital. It’s an invitation to have our bones screened and if there is a hint of some bone thinning we will be offered a bisphosphonate, a drug for osteoporosis.
4). This advert for a bisphosphonate, then an expensive new drug, conveys the impression these drugs work just like the plate put in my shoulder – good for the patient, her family and friends – a treatment that pays for itself.
Guidelines recommended these drugs. The companies making them provided free bone scanners for screening programmes.
But these drugs don’t work like the plate in my shoulder, leading to a need for auditors and managers to get this service working right. We pay for the screeners, auditors and managers to put drugs in people’s mouths – not Pharma, which leaves a grinning Pharma asking What do you mean our drug costs are high? The drugs budget remains a constant 10% of health expenditures.
5). This is before we start paying for the problems these drugs cause like the spiral fracture of the femur in this X-Ray. Before the bisphosphonates these were rare. Now faced with a fracture like this, we immediately know the patient has been on a bisphosphonate. Drug companies claim these fractures are anecdotal because no RCTs have ever shown this happening – you have to have been on the drugs for years for this to happen and trials don’t extend that long – but the RCT data which no-one gets to see shows there is no drop in fracture rates on bisphosphonates.
Abnormally thickening bones is a risky thing to do. Better to encourage people over 50 to remain fit and keep active. Telling them they have bone thinning encourages them not to cut the garden, not to be active, and take pills instead.
Companies and politicians have a get out clause for the increasing costs of healthcare – ageing. This seems to make sense – surely, we need more services as we age?
6). This obvious idea is wrong. Here you see Bart Simpson being told by Homer ‘pull yourself together kid’. These days Bart is more likely to get an antidepressant. There are two points here. One is that we have lost wisdom.
7) Second the process you saw in osteoporosis is being replicated in children’s mental health. The government is pumping more money in – for screeners, auditors, managers and psychotherapists to put antidepressants in our children’s mouths but things are clearly not working out leaving Jeremy Hunt, a recent Minister for Health in the UK, saying children’s mental health services are the greatest point of failure in the NHS.
There have been 30 RCTs of antidepressants in depressed children – all negative – even the RCTs that led to Prozac being licensed for children. This is the greatest concentration of negative trials for anything ever – but despite this, antidepressants are now the second most common drug being taken by teenage girls. What’s going on.
Well the literature on antidepressants is almost entirely ghost written and there is no access to the data from antidepressant trials.
8). Ghostwriters don’t look like this. They are mostly women with PhDs.
9). Here is one page of a Pfizer document showing the preparation of articles on their SSRI Zoloft. Two trials have been done on PTSD. The trials in fact show Zoloft didn’t work but both were written up as positive – one to appear in the New England Journal of Medicine and the other in JAMA – the premier journals in the field. Most of us would figure articles in journals like these must be true.
On the left you see ‘author – TBD’ – to be determined. The articles are written – the company will later pick authors based on who would suit the marketing profile of the drug.
For 30 years the greatest concentration of Fake News on earth has centred on the drugs a doctor gives you – whether psychotropic drugs, statins, or heart drugs.
10). Many good people are concerned about corruption in medicine – the free pens, lunches, conflicts of interest and lack of Transparency. I think this ghostwriting and lack of access to trial data – let’s call it Cisparency – is more important.
But there is an even deeper problem – your belief that Randomized Controlled Trials, if done by angels of course, are the answer to our problems. Your belief is our problem.
11). The first use of randomization in a trial was in the 1948 MRC study of streptomycin run by Tony Hill. This was British medicine’s 1966 World Cup moment – the academic media still dwell on it lovingly and lose sight of the fact that streptomycin had been evaluated in the Mayo Clinic 2 years earlier and this evaluation told us things about streptomycin the MRC trial missed – that some patients became tolerant to it and others had hearing loss.
12). Hill didn’t practice medicine – but here in 1965 even he is saying:
“Frequently with a new discovery… the pendulum at first swings too far… Given the right attitude of mind, there is more than one way we can study therapeutic efficacy.
Any belief the controlled trial is the only way would mean not that the pendulum had swung too far but that it had come off its hook”.
He at least was very aware that RCTs could be helpful but their place was limited – to a primary efficacy endpoint. They are not a good way to evaluate a drug overall.
13). In the late 1950s Louis Lasagna was the major advocate of RCTs but to little effect.
14). The current premium we put on RCTs stems from the thalidomide crisis. In the wake of this, politicians had to be seen to do something and in the USA in 1962 they amended the Food and Drugs Act to require companies to demonstrate efficacy in addition to safety. How would they demonstrate efficacy? Up popped Lasagna saying RCTs would do the trick.
15). At this point, there had been only one drug put through a placebo controlled RCT before being brought onto the US market in which it had been shown to be effective and safe. That drug? Thalidomide – in a trial run by Lasagna.
16). Lasagna like Hill soon began to appreciate the limitations of RCTs.
Here in 1983 he is responding to an article about adverse events that claimed that:
“Spontaneous reporting is “the least sophisticated and scientifically rigorous . . . method of detecting new adverse drug reactions”.
With:
“This may be true in the dictionary sense of sophisticated meaning ‘adulterated’ . . . but I submit spontaneous reporting is more ‘worldly-wise, knowing, subtle and intellectually appealing’ than grandiose, expensive RCTs”.
17). And a few years later he had the following to say:
“In contrast to my role in the 1950s which was trying to convince people to do controlled trials, now I find myself telling people that it’s not the only way to truth.
“Evidence Based Medicine has become synonymous with RCTs even though such trials invariably fail to tell the physician what he or she wants to know which is which drug is best for Mr Jones or Ms Smith – not what happens to a non-existent average person”.
18). The person responsible for randomization and the linked use of statistical significance testing in trials was Ronald Fisher, whom you see here smoking – he didn’t believe the evidence that smoking caused lung cancer.
19). Fisher never trialled anything. He ran a thought experiment about experiments. If someone knows what they are doing, the only things that can interfere are some confounder they don’t know about or chance. Randomisation takes care of the confounder and we can agree that 1 wrong result out of 20 is down to chance. If we know what we are doing Robin-Hood-like we should get the same answer every time – as the image shows.
20). But no RCTs for anything in medicine looks like that – they look like this. In the case of the antidepressants its sheer chance a patient put on one is going to be helped. These RCTs have no anchor in the real world. They do not offer gold standard knowledge – but landing an arrow anywhere on this target is the standard through which companies make gold – which is why you think RCTs rather than your own view offer gold standard clinical knowledge. Companies don’t have to let anyone see the arrows that totally miss the target.
21). This is all blindingly obvious. But we’ve had a denial mechanism in place since before the Berlin Wall came down, with statisticians and journals like the BMJ saying “Hey no-one uses p-values anymore – we use confidence intervals”.
Here on a pre-Euro Deutschmark, you see Carl Friedrich Gauss, who in 1810 created the confidence interval and the idea of measurement error. The problem he solved was that 10 astronomers looking at a star – given the instruments then – came up with 10 different locations. Were they seeing just the one star or several? Gauss’s answer was that if the observation lay outside a normal distribution curve it likely came from a different star.
But if I take 10 or 20 of you here and gave you a drug that would sedate some of you, or cause your heart rate to slow, others will find themselves unable to sleep or their heart rate speeded up. This is not measurement error. Applying confidence intervals to these data risks concluding these drugs have no effect on heart rate or level of sedation.
Neither p-values, nor confidence intervals, as applied to clinical trials have an anchor in the real world. Let me show you.
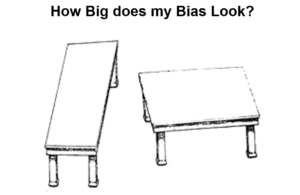
22) RCTs are supposed to control even the confounders we don’t know about. But they routinely introduce confounders. If you print off this slide and superimpose the table tops you will end up confounded – they are the same size. Despite doing this, they will still look different here and my problem may be that even after hearing what you hear next you will still think that RCTs give us the right answer about drugs.
23). Imipramine was the first antidepressant. It is more potent than any SSRI. It can cure melancholia – a severe depression that leads people to commit suicide. But imipramine itself can cause people to commit suicide. Nevertheless, putting this drug that can cause suicide into a trial of melancholic patients I’d expect that fewer people given imipramine would go on to suicide compared with people given placebo. We’d conclude this drug protects against suicide not that it causes suicide.
24). In contrast, the trials that brought SSRIs on the market show an increase of suicidal events on SSRIs compared to placebo. This is because the trials had to be done in mildly depressed people and so the drug risks showed up more clearly.
25). If imipramine was put into trials of the same patients it too would seem to cause suicide. We call these drug trials, but they aren’t – they are treatment trials. A drug trial would be done in healthy volunteers. Second, clinical RCTs tell us nothing about cause and effect.
26). And where both treatment and condition can cause superficially similar effects, which happens in most medical trials, you are completely unable to tell what is going on. I’m sure you can all add to the list here.
27). Now take this GlaxoSmithKline document. In these placebo-controlled trials you see 11 suicidal events on paroxetine versus 0 on placebo. This is a problem for the company – so much so they have omitted at least one event from these trials and complete trials.
28). But they also did trials in intermittent brief depressive disorder – also called borderline personality disorder – where patients engage in suicidal events much more frequently than in classic depression. Now the data for paroxetine don’t look good here either – and the real data are worse – we could add 12 extra suicidal events on paroxetine here and still get the same magical result you see on the next slide.
29). When you add the two groups – Hey presto – Paroxetine protects against suicide. This is using a problem a drug causes to hide a problem a drug causes. You can get the same confounding effect every time the condition being investigated is heterogenous – as is the case for depression, diabetes, parkinson’s, breast cancer, back pain and pretty well every condition we treat.
30). Now what you often hear about adverse events is that of course RCTs can miss idiosyncratic events or events too rare to be picked up in say 200 people. This is clever propaganda and wrong. Whatever sex, age, ethnicity you are, pretty well everyone here given an SSRI would have some genital numbing 30 minutes after a first dose. This is the commonest effect these drugs have.
31). The best example of how RCTs introduce confounders starts here with Frank Ayd, who before 1962 discovered amitriptyline – the best-selling of the first generation of antidepressants – a good treatment for melancholia which causes loss of libido. Unencumbered by RCTs, Ayd was able to say within a year of amitriptyline being in use that it caused sexual dysfunction.
32). A decade later, George Beaumont, working for Ciba-Geigy had the job of marketing clomipramine, now recognised as our most potent antidepressant, but then another molecule in a crowded field. He placed articles in newspapers featuring a minor celebrity, thrilled that her boyfriend’s premature ejaculation problem could be managed by 10 mg of clomipramine taken 30 minutes before intercourse – the standard antidepressant dose is 150 mg
33). The SSRI antidepressants, derived from clomipramine, were launched around 1990. SSRIs are ineffective for proper depression, but this is rare compared to the nervous problems for which doctors were giving benzodiazepines. The SSRI marketing need was to transform cases of Valium into cases of Prozac – transform people with no sexual dysfunction treated with pills that had no sexual effects into people who were depressed.
Doctors began to hear they could be sued for prescribing benzodiazepines which cause dependence. The real need they were told was to treat the underlying depression, with antidepressants, which do not cause dependence, rather than treat the superficial anxiety with dependence producing drugs.
Prior to marketing, companies ran phase 1 studies of SSRIs. In these healthy volunteers became dependent after two weeks and were left anxious and depressed afterwards. Within 3 years of paroxetine being on the market, there were more reports in Britain about dependence on it than there had been in 20 years from all benzodiazepines combined.
The initial labels for all SSRIs stated that less than 5% of patients in clinical trials reported sexual dysfunction. But in some phase 1 trials, over 50% of healthy volunteers had severe sexual dysfunction that in some cases lasted after treatment stopped.
How does over 50% become less than 5%? Well in RCTs investigators focus almost entirely on the primary endpoint – does the drug work – with minimal space and time to record adverse events. They are unlikely to record a problem, in particular one that can be passed off as a feature of the illness.
The bias here is total. The single commonest effect of these drugs – not a rare effect RCTs might miss – has vanished. Surely, it’s still there in the real world – what real world?
34). In 2006, PSSD – Post SSRI Sexual Dysfunction – emerged. My first encounter with this was when a lady in her 30s presented to me 20 years ago telling me she was unable to function – I said this will clear once you stop your SSRI. No she said – she’d been off treatment for 3 months and she could take a hard-bristled brush and rub it up and down her genitals and feel nothing.
Turns out the first reports of PSSD had been reported to MHRA in 1991. They have hundreds. The first academic publications came in 2006. This is a state where people become profoundly genitally numb and lose the ability to orgasm properly and lose libido. It may start on the drug but typically gets worse after treatment stops. It can endure for years or in some cases forever. Some kill themselves, others refer themselves to Dignitas.
Almost identical problems have been reported after finasteride and isotretinoin. This is a pharmacological and neurological mystery – whose solution is worthy of a Nobel Prize.
35). But despite PSSD, the sexual problems on antidepressants have vanished. In May this year BMJ featured an article on Declining Sex in Britain. It fingered depression as the cause for this – no mention of antidepressants even though antidepressants almost universally cause this while the nervous problems for which they are given don’t cause sexual dysfunction and the benzodiazepines didn’t cause sexual dysfunction either. The media were completely uninterested to pick up the treatment issue – even though between 10-15% of us are on these drugs – because we can’t stop – which means 20% of us are not making love the way we might want.
36). The medical response to PSSD is – don’t be stupid a drug can’t have an effect if it’s not in your body. There is no real evidence for this. If you google this, you’ll be ill forever. Maybe you have some past trauma that counselling or an antidepressant could put right. The ridicule and lack of any recognition contributes to the suicides.
So we figured on petitioning EMA to get this problem included in the label of drugs. Why would EMA budge in response to us given they are sitting on thousands of reports of just this problem since the early 1990s and have done nothing?
37). The unfortunate experience of Walter Raleigh suggested a way forward. In 1618 Raleigh was executed in London on the basis of hearsay – people saying things about what he had said or did without coming to court to be cross examined. After his execution legal systems worldwide changed so they don’t now admit hearsay evidence. People have to come into court to be cross examined.
Now if you report an adverse event to the regulator, the regulator will remove patient names – transforming the report into hearsay and making it impossible to establish causality. Examining or cross-examining the patient is crucial to establishing causality. Without this, regulators can accumulate tens of thousands of reports and do nothing.
Companies, in contrast, are legally obliged to chase a patient’s medical records. They do so to find out if you had an ingrown toenail at the age of 2 that might explain why you are unable to function sexually post SSRI – if they can’t find anything they often conclude their drug has caused the problem and include it in the drug label but with words that most doctors perceive as not conceding cause and effect when in fact they are conceding causality.
If we want to restore healthcare, we and our patients have to insist our names are left on the reports and as things stand we should report to companies not regulators. We have to make clear we are willing to come to court to be cross examined if need be. The legal system cannot dismiss reports from people willing to come into court to be cross examined. The question is – how many of you have the courage to do this?
38) The alternate lecture to this one ends with an Economics is from Mars, Medicine from Venus slide. Aimed at persuading you that anyone who works in health knows more about neo-liberalism – its good and its bad – than any economist or politician.
39). Algorithms are from Mars and Magic from Venus pitches algorithms – tools that work in clearly defined ways that be capitalized – as the basis for economics. RCTs are a great example of an algorithm and EBM a compelling slogan for an algorithmythology that is incompatible with medicine.
You are better at evaluating a drug than any RCT. RCTs can’t offer anything to the Magic central to medicine which involves a decision about whether to attempt to bring good out of the use of poison or a mutilation. But RCTs can be capitalized, and your discretion can’t, and this pits us against them. At the moment – they are winning
When a patient consents to a poison or mutilation, key to the possibility of magic and their subsequent life is the relationship between them and you. If they can trust you, if they sense you would do the same for yourself or your child as you are offering them, you gain social capital. When you give a poison, if you betray them – if they sense you would not have taken that bisphosphonate – you lose that capital.
Taking a poison at our suggestion remains one of the best ways to discover new treatments. But in addition, PSSD for instance is a complete pharmacological and neurological mystery, the answer to which might lead to a Nobel Prize but even more important to most of us could shed a lot of light on who or what we are.
We need a Relationship Based Medicine rather than Evidence Based Medicine to grapple with mysteries like this.
Excellent, as usual! Not many could put across these serious issues in such a homely way. I marvel at the way that you can change your language to suit your audience BUT THE SAME MESSAGE IS THERE LOUD AND CLEAR.
Now to your audience. I take it there was a Q&A session once the recording was done? How did the audience react? Two walked out, as we saw (maybe with good reason) – I fail to see how anyone could walk out, unless in a crisis!, as, from beginning to end one is left wondering what new facts you are about to present.
Knowing that these same facts have now been presented over the course of a few years – plus or minus a few facts as time/audience changes – how is it that so few ACKNOWLEDGE what you have to say or are willing to admit that they know who you are, even if they don’t like what you say?
Do you feel that, at the time of giving a lecture/ talk, that you are winning over an audience and that they, on returning to their life outside the lecture hall, forget all about it? Or is it pressure in the workplace that causes them to put all that they heard to one side? I know that I keep referring to the times when you came to Prestatyn, but there the majority were amazed, shocked and believed – and are still talking about points that you made. There were two who come to mind who didn’t see eye to eye with what you had to say – both professionals, either in the medical world or involved with drug trials. That leads me to feel that the ‘blockage’ is to do with ‘brainwashing in the workplace’! It is also why I feel so strongly that the only way to move forward may well be to keep ‘ordinary folk’ topped up with these messages whenever possible.
The talk was in a hospital setting so some people will have been bleeped out. The Q & A was constructive. Clearly one of the themes will always be, well what do we do now and I don’t have or am not going to provide an answer for that.
Will it make any difference – no. It takes too many people beyond a critical comfort zone. The trouble is there is no ready point of compromise. Do we encourage people to trust their own judgement or don’t we – there isn’t a half-way on this one
D
I’m not sure that I can see an option – we’ve trusted the ‘professionals’ for so long only to find out that, in many instances, we were given false hope therefore it’s time to think for ourselves. That, to my mind, doesn’t mean that we don’t rely on expert knowledge to some degree, rather it means that we enter into a dialogue with the ‘professionals’, question matters that we don’t understand, share concerns that we may have regarding medications etc. The days of ‘them’ and ‘us’ should be gone – we must work together, us with them and them with us, all with one aim of improving standards of care. Maybe doctors NEED to see that we are fast waking up to what is going on ( and has gone on for far too long) and are no longer willing to meekly carry on with their suggestions of what is best for us.
One question I would love an answer to is – how on earth do YOU carry on? Each lecture or talk that you give feels like the first time you’ve given it, as if you’re sharing some ‘new found truth’. You’ve been sharing the basics for many years now – adding new bits as they become relevant and yet the presentation continues to have the same energy time after time. It must be hard work – but much appreciated. Without your show of energy, I guess ours would have long disappeared too!
It would be fine and dandy if the RCTs shown were put in to the boiling cauldron of a court of law. In the UK we have never taken a pharmaceutical company to court over a defective product. Not for want of trying.
It will seem unbelievable that the law operates in mysterious ways and despite overwhelming evidence, that points of law come before the actual frauds committed. Since thousands have been catastrophically injured with Paroxetine, 67,000 emails to Panorama, all those years ago.
http://news.bbc.co.uk/1/hi/programmes/panorama/3154053.stm
This puts Paroxetine in a peculiar position.
As I see it, the view is that lectures like this are for informative learning about RCTs and ghostwriters and the mountains of information that they should know. To make them think and realise that the undercurrents of SSRIs don’t make them the hale and hearty helper they are perceived as being.
The Petitions by Marion Brown and Stevie Lewis. PHE and RCP reluctantly giving a little noise. NICE rewriting guidelines. Necessary steps.
But they don’t address the fraud by GlaxoSmithKline having got approval for Paroxetine with shady write-ups, distorted RCTs and 329.
All these years and no-one speaks about “Betrayal and Social Kapital” quote, Grand Round, and, K, a special K…
Of course, it might have occurred to David’s audience, if that is the case with Paroxetine, why hasn’t there been a hue and cry.
So all those who could talk about this ‘No-Show’, don’t.
Those in high places; GSK will not form to their lips.
Interestingly, the Government Chief Scientist is quoted as saying, yesterday –
“But that’s still horrible, it’s still an enormous number of deaths and an enormous pressure on the health service, and having spent twenty years as an NHS consultant as well as an academic, I know what that looks and feels like.”
https://www.fiercebiotech.com/special-report/patrick-vallance-glaxosmithkline
As more than one research expert noted, Glaxo ($GSK) has been feeling the heat of blistering criticism for its past secretive ways. Bold action was required to help counter an increasingly dour public image, and Vallance has played a leading part in the drive to change the public’s perception of GSK.
So, lots to talk about … in the ‘Grand Round’ of things …
Cherry-picked … ”did not apply any bias either”
‘It’s clear that GSK does not do that and the medical journals did not apply any bias either.’
Setting the record straight…
Sharing our trial results, regardless of whether they reflect positively or negatively on our medicines is the right thing to do.
https://us.gsk.com/en-us/behind-the-science/how-we-do-business/setting-the-record-straight-why-we-publish-data-both-positive-and-negative/
Patrick Vallance, President, R&D commented: “The results of this analysis allow us to challenge perceptions that pharmaceutical companies cherry-pick what is submitted for publication according to favourability towards their medicines. It’s clear that GSK does not do that and the medical journals did not apply any bias either. These results reinforce our strong belief that the scientific community can derive as much, if not more, insights from negative data as positive data, and we must continue to ensure access to all of our clinical study data involving patients, with the aim of ultimately benefitting patients”.
With Transparency Pledge, Glaxo Makes Promises No Other Drug Company Has
Matthew Herper Former Staff
https://www.forbes.com/sites/matthewherper/2012/10/11/with-transparency-pledge-glaxo-makes-promises-no-other-drug-company-has/#e59d7b64b90b
Putting GlaxoSmithKline to the test over paroxetine
BMJ 2013; 347 doi: https://doi.org/10.1136/bmj.f6754 (Published 12 November 2013) Cite this as: BMJ 2013;347:f6754
Blockbuster antidepressant paroxetine is no stranger to headlines. The drug is now back centre stage as requests for clinical data from one of its trials are testing manufacturer GlaxoSmithKline’s commitment to full transparency,
Peter Doshi reports
https://www.bmj.com/content/347/bmj.f6754
Below is the exchange of letters between Jon Jureidini and GlaxoSmithKline between April 26 and November 8, 2013, in which Jureidini requests data from paroxetine study 329.
https://www.bmj.com/content/347/bmj.f6754/rapid-responses
Jorge Hernán Ramirez
Professor of Pharmacology
Universidad del Valle
‘Concerns expressed by other authors, regarding the efficacy and safety of antidepressant drugs in humans, are legitimate and well-founded.(3,4) The evidence in peer-review medical journals supporting the efficacy and safety of antidepressants in humans have been cherry-picked.’
But bear in mind also that the cost of vaccinating a single child according to the schedule has gone up by more than a hundred times since the beginning of the millennium.
https://www.bmj.com/content/366/bmj.l5576/rr-4
The biggest spoke that Andrew Wakefield threw into the emergent project in 1998 was to suggest that parents might want to continue to pick and choose with single vaccines when the project required multivacs – which in themselves were a tool against choice. Of course, even by the standards of the pharmaceutical industry testing of vaccines was rock bottom, while compliance was all – the effort to remove choice is the pursuit of the millennium. Child health on the other hand is not so good. “Forwards, not backwards!” as Tony Blair used to say.
Talking of vaccines, and the present apparent rush to find one to stop the spread of Covid -19, what will we do? Will we stand strong and refuse it? Will we spread the word about the dangers of the substances within it ( if we know them)? Or will we oblige and turn up for our jab?
Maybe more to the point – WILL WE HAVE A CHOICE? If we DON’T have a choice, how can we ensure that EVERY SINGLE PERSON has that right of choice taken away from them? We cannot allow ‘them’ to follow one rule whilst ‘they’, who are deemed superior, decide what is ‘good enough for the majority’ as, unfortunately, ‘good enough’ hardly ever is that.
Mary
It is a very interesting and troubling point. In 2009 the Department of Health in the UK only managed to persuade about 10% of the population (~6m people) to accept Pandemrix although they had ordered 132m rounds.
https://www.bmj.com/content/364/bmj.l1259/rr
Of course, by that stage everyone thought the swine flu pandemic was pretty much a farce, but it does not actually follow when people are offered new vaccines in Africa for scary diseases like Ebola or Malaria that the immediate reaction is one of trust either. If, of course, the government try and force the new vaccine on people the trust will be even less, though I see for instance the Danish parliament have already legislated for it and thrown mandates for the established schedule opportunistically into the emergency legislation as well, in a great fit of communal virtue-signalling.
Alas, even with a decade’s development the prospects for a non-lethal, effective SARS-CoV-2 vaccine would be virtually infinitesimal. It is wrong to tell people there will be one in 12/18 months, and even scarier if “they” actually mean it.
https://www.linkedin.com/pulse/moderna-us-niaid-poised-endanger-world-population-james-lyons-weiler?trk=portfolio_article-card_title
Thanks John – this rush for a vaccine is the part that I find most worrying. I have a niece who is a medical statistician at a UK Uni., now working from home, whose workload is greater than ever because of all the work that’s being done by different groups at the Uni “on the science of Covid-19”. ‘The way to go far is by going slowly’ needs to be their motto I guess!
Mary
I think we need to make sure we have optimal natural immunity (nutritional etc).
Latest from Children’s Health Defense (Lyn https://childrenshealthdefense.org/news/dr-fauci-and-covid-19-priorities-therapeutics-now-or-vaccines-later/?utm_source=mailchimp
Pandemrix vaccine: why was the public not told of early warning signs?
BMJ 2018; 362 doi: https://doi.org/10.1136/bmj.k3948 (Published 20 September 2018) Cite this as: BMJ 2018;362:k3948
https://www.bmj.com/content/362/bmj.k3948.full
Eight years after the pandemic influenza outbreak, a lawsuit alleging that GlaxoSmithKline’s Pandemrix vaccine caused narcolepsy has unearthed internal reports suggesting problems with the vaccine’s safety. Peter Doshi asks what this means for the future of transparency during public health emergencies
In October 2009, the US National Institutes of Health infectious diseases chief, Anthony Fauci, appeared on YouTube to reassure Americans about the safety of the “swine flu” vaccine. “The track record for serious adverse events is very good. It’s very, very, very rare that you ever see anything that’s associated with the vaccine that’s a serious event,”1 he said.
Four months earlier, the World Health Organization had declared H1N1 influenza a pandemic, and by October 2009 the new vaccines were being rolled out across the world. A similar story was playing out in the UK, with prominent organisations, including the Department of Health, British Medical Association, and Royal Colleges of General Practitioners, working hard to convince a reluctant NHS workforce to get vaccinated.2 “We fully support the swine flu vaccination programme … The vaccine has been thoroughly tested,” they declared in a joint statement.3
Except, it hadn’t. Anticipating a severe influenza pandemic, governments around the world had made various logistical and legal arrangements to shorten the time between recognition of a pandemic virus and the production of a vaccine and administration of that vaccine in the population. In Europe, one element of those plans was an agreement to grant licences to pandemic vaccines based on data from pre-pandemic “mock-up” vaccines produced using a different virus (H5N1 influenza).
Another element, adopted by countries such as Canada, the US, UK, France, and Germany, was to provide vaccine manufacturers indemnity from liability for wrongdoing, thereby reducing the risk of a lawsuit stemming from vaccine related injury.45
In …
https://www.bmj.com/content/362/bmj.k3948/rapid-responses
Thomas Breuer
Chief Medical Officer, GSK Vaccines
‘We are concerned that publications such as the one in the BMJ could generate undue concern and negatively influence trust in vaccines and vaccination. GSK remains firmly committed to transparency of safety information but calls upon the scientific community, including the publications that serve that community, to ensure that the disclosure of such information is driven by scientific responsibility and integrity.’
I also think we need to urgently look at therapeutic solutions for this disease – I have just seen the highly successful results of an obviously small trial combining hydroxychloroquine and azithromycin. Things do seem to be spinning out of control. On Italy’s worst day on Saturday 561 people died of Covid-19 related illness in Lombardy which has a normal death rate of only 250-300 people a day.
https://i.imgur.com/7TtEbEW.jpg
https://en.wikipedia.org/wiki/2020_coronavirus_pandemic_in_Italy
The Coronavirus Outbreak
Gilead Withdraws Request for Special Orphan Status on Experimental Virus Treatment
Critics said the company was profiteering from the coronavirus pandemic by seeking tax and monopoly benefits under a program intended to encourage drug development for rare diseases.
Credit…David Paul Morris/Bloomberg
By Katie Thomas
March 25, 2020
Bowing to criticism that it was exploiting the coronavirus pandemic, the drugmaker Gilead said on Wednesday that it would no longer seek orphan-drug status for remdesivir, an experimental drug that is being tested as a possible treatment.
The Food and Drug Administration had only granted the special designation on Monday — which gives drug companies a seven-year monopoly on sales, tax credits and expedited approval. Gilead said it asked the agency to rescind the status.
The company’s decision to seek orphan status for the drug had drawn immediate criticism. Senator Bernie Sanders of Vermont, who is seeking the Democratic presidential nomination, called it “truly outrageous,” noting that Gilead had received “tens of millions” of dollars from the federal government to develop the drug.
The consumer group Public Citizen and other health groups sent a letter on Wednesday to Gilead’s chief executive, Daniel O’Day, asking him to reverse course. “This is an unconscionable abuse of a program designed to incentivize research and development of treatments for rare diseases,” the letter said. “Calling Covid-19 a rare disease mocks people’s suffering and exploits a loophole in the law to profiteer off a deadly pandemic.
No treatment has been proved to be effective against Covid-19, the disease caused by the coronavirus, and Gilead is just one of several companies with drugs in trials around the world. More than 438,100 people have been sickened in at least 168 countries, according to official counts. As of Wednesday afternoon, at least 19,641 people had died.
The Orphan Drug Act, passed in 1983, was intended to encourage development of drugs that treat diseases affecting fewer than 200,000 people in the United States. But in recent years, drug companies have been accused of exploiting the law to reap millions, if not billions, in sales. Companies have gotten orphan designation for products that were already blockbusters, including Humira, which has long been the world’s top-selling drug.
Without orphan-drug status, a company like Gilead would receive five years of monopoly protection for a new drug approval.. A drug like Gilead’s remdesivir or another treatment could ultimately be administered to millions of people around the world over the course of the pandemic.
In a statement, Gilead said it had sought the orphan status to expedite approval of the drug, in particular a required pediatric study plan that, without such a designation, the company said could have taken up to 210 days to complete. But Gilead said that after speaking to regulators, it was confident the application would move quickly.
“Gilead recognizes the urgent public health needs posed by the Covid-19 pandemic,” the drugmaker said. “The company is working to advance the development of remdesivir as quickly as possible and will provide updates as they become available.”
Peter Maybarduk, the director of a Public Citizen program that advocates for global access to medicines, rejected the company’s argument that the requirement that it complete a pediatric study plan — which would be waived with an orphan designation — would have slowed the process. “We have to know whether a drug may affect children differently than adults,” he said. “Gilead should not have been looking to skip this step in the first place.”
Remdesivir is being studied in several large-scale clinical trials around the world, including in a huge trial announced last week by the World Health Organization. But the results have not been reported yet, and it is still unclear whether the drug works against the coronavirus. It was studied to treat Ebola, but it did not work well enough against that virus.
Last week, President Trump promoted the drug as one of a handful that might work against the coronavirus. Gilead has been inundated with requests for “compassionate use” access to the drug from doctors with dying patients who are desperate to try anything that might help.
This past weekend, Gilead said that the overwhelming demand had created a backlog and that it was switching from approving access on a case-by-case basis to a system in which patients would be approved in large groups. But that new program has not yet gotten underway, leaving some doctors and patients scrambling. A Gilead spokeswoman said on Wednesday that the company’s goal was to have the broader program up and running at some sites in the United States this week, with others to come after that.
Around two weeks ago the power to be given to police was being described as powers of ‘sectioning’ members of the public It was not coupled to mental health. The word ‘sectioning’ has now disappeared relating to the public in general and replaced with powers to ‘arrest’. The suggestion that powers to section those who opposed authorities using a mental illness tag had obviously been flagged up It is is a stark reminder of what happens in totalitarian states . But People who do have mental health issues are going to be in a perilous position with these new powers already in force from today. The increase in forcible medicating is more than likely along with increase in sections.
PUBLISHED: 16:54, 25 March 2020 | UPDATED: 21:35, 25 March 20
Emergency coronavirus powers are set to come into law after being approved by Parliament today.
The Coronavirus Bill passed its final legislative hurdle this afternoon after it was approved by the House of Lords.
The changes include reducing the number of doctors required to sign off on sectioning those with mental health issues from two to one, while police would be given authority to force those infected with Covid-19 to self-isolate, with the threat of four-figure fines for refusing to be tested.
After just two days of debate in the upper chamber, the fast-tracked Coronavirus Bill was given an unopposed third reading by peers today. It then received Royal Assent from the Queen late this afternoon.