A distinguished colleague (C1) introduced last year’s word of the year – AI Slop – into last week’s The Prozac Liberation Front post.
As an unaccountable editor, I took the liberty to suggest that many of us seemed to figure – or would pretty soon get round to figuring – that AI was all too likely to go the way of the Internet as a potentially democratising force in healthcare. If it can turn the Wine of decent human interaction into healthcare Water, the consequences for every other less intimate and personal domain of our lives were likely to be even worse.
At the heart of our dilemmas is that health has always been a Liberal and Socialist bastion in which people who cherish liberty on their own part, or on behalf of what the call the ‘people’, hold out against the powers that be – Can We Avoid Being Eaten.
The worry for some (Liberals) has been that the collective in the form of a bureaucracy (Now in US English called a Deep State) would squash individual liberty just as effectively as an aristocracy had or an oligarchy seems likely to do.
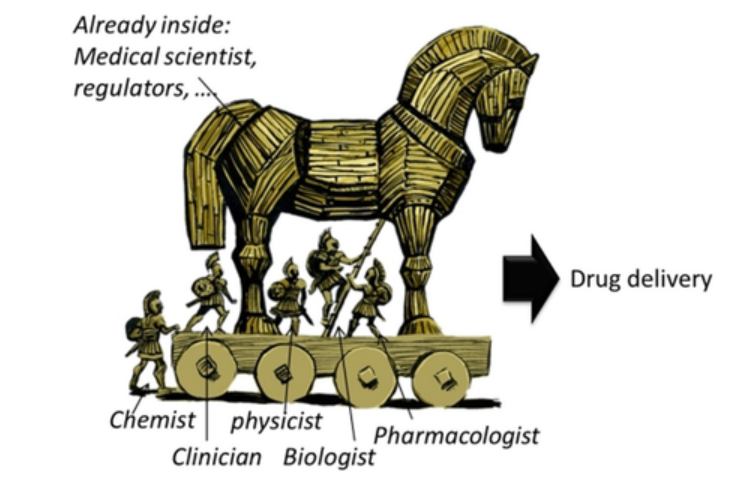
The bigger unnoticed worry is that the advent of effective pharmaceuticals, which looked like they might free us up to better live the lives we wanted to live, has enabled Companies (Deep State Corporate Bureaucracies) to effect an entry into the citadel of our liberties by means of a Horse – Randomized Controlled Trials (RCTs).
 T
TThese Averaging Machines not only get invaders into the city but get everyone to swallow the meds – not just those who might respond. RCTs are also the Gold Standard way to Average Hazards out of Existence.
Large Language Models (LLMs) are also Averaging Machines and with an algorithim or two inserted into screens here or there will ensure that only the messages from company RCTs get heard. It seems inevitable that LLMs will buttress rather than undermine Deep States.
Is there an Achilles Heel be found? Perhaps not, but there is scope for amusement in the meantime.

Britain’s medicines regulator is MHRA, who you could say are the Still Heart of a Beating UK Healthcare World – just to be clear Hearts are still when dead. But in their afterlife, bureaucrats will continue to seem to do something as a cover for doing nothing. Hence a Document proclaiming a Revolution.
Project overview
Your health decisions matter. The information you receive about your medicines should be clear, accessible, and support informed conversations between you and your healthcare professional. The MHRA is committed to leading an inclusive approach to improving medicines information.
To achieve this, we have launched the Improving Patient Information project, to work closely with stakeholders across the health system including patient groups and charities to understand barriers and identify how information can be made more accessible, trusted, and future-fit.
Our aim is to ensure that patient information for medicinal products is clearer, inclusive, and easier to understand. This will be achieved by placing patients at the centre of the project.
A major focus of this work will be improving access to patient information leaflets in the UK through the use of digital solutions.
The Improving Patient Information project has a three-phase approach to delivery:
- Phase one (April 2025-March 2026): Scoping phase focused on engaging with stakeholders across the health system, understanding how patients access patient information and proposing an action plan
- Phase two (2026-2027): Establishing a multi-stakeholder governance structure and collaborating with partners across the healthcare system to deliver the action plan
- Phase three (2027-2028): Reviewing the impact of action plan, developing a strategy for implementation.
We have five design principles to guide our work: patient centred, accessible, trusted, innovative, and standardised.
Research reports
Woodnewton Associates was commissioned by the MHRA to conduct independent research on the role that patient information leaflets provide to informing patients. The findings and recommendations presented in this report are those of the researchers and do not necessarily reflect the views of the MHRA.
- Title Research conducted on the role that patient information leaflets provide to informing patients
- Details A research report defining the current baseline for patient engagement with and accessibility of patient information leaflets.
- This research was commissioned and funded by MHRA. Its aim is to provide evidence that will help inform future changes to patient information to make it more accessible, trusted, and fit for the future
- Our action plan is based on evidence we have gained through this research.
WN Report: Research on the Role of Patient Information Leaflets in Meeting the Information Needs of Patients
Smile and the World Smiles With You
Ron Law, a Risk and Policy Adviser based in New Zealand – perhaps the most active person on another listserve on which Prozac Liberation ran – responded that ChatGPT could have its uses – for making cartoons. This is absolutely true as the recent set of 4 RxISK videos with 2 more to come shows. He also figured, with a touch of guidance, it was good for Drafting Reports.
Knowing he loves nothing more than tackling regulators, I sent him the link to the MHRA document and was astonished to get a fabulous response within minutes.
A Most Welcome Commitment to Clarity
It is, of course, most heartening to observe the MHRA’s newly invigorated commitment to “clear, accessible, and trusted” patient information. One could scarcely object to an initiative so impeccably phrased, nor to the proposition—advanced with commendable solemnity—that patients ought, in principle, to understand the medicines they are invited to consume.
A Brief Encounter with Institutional Memory
However, for the more historically minded observer, this sudden institutional enthusiasm for transparency does invite a certain… reflective pause.
For it was not so very long ago that the same regulatory architecture appeared to exert itself with quite remarkable vigour in the opposite direction—namely, in the careful management, dilution, or deferment of information concerning potential harms associated with both COVID-19 vaccines and SSRI medicines. One recalls, for example, the rather strenuous reluctance to foreground adverse event signals in a manner that might have been considered “clear” or “accessible” to the uninitiated patient, let alone “conducive to informed decision-making.”
Indeed, the prevailing philosophy at the time might best be described not as patient-centred transparency, but as professionally mediated reassurance — wherein information was filtered through a series of interpretive layers designed to ensure that what reached the patient was not so much the unvarnished evidence as its more palatable administrative rendering.
The Damascus Conversion
In that context, the MHRA’s apparent road-to-Damascus experience is nothing short of remarkable. One is bound to admire the speed and completeness of the conversion. Yet it does prompt a delicate question regarding its precise point of origin. Was this newfound devotion to transparency born of accumulated evidence, external scrutiny, reputational necessity, or merely the natural lifecycle of regulatory fashion? The chronology, if one were unkind enough to examine it closely, may suggest that this enlightenment is rather more recent—and rather more convenient—than the rhetoric implies.
Trust, or the Management Thereof
The present declaration of intent—to place patients “at the centre of every stage” and to ensure information is “trusted” and “fit for the future”—thus carries a certain quiet irony. One is tempted to ask whether “trust” is here conceived as a product of fuller disclosure, or as the outcome of more sophisticated presentation.
Equally intriguing is the emphasis on “digital solutions,” which, while no doubt modern and efficient, may also offer unparalleled opportunities for the dynamic curation of information—allowing inconvenient complexities to be rendered, shall we say, less immediately conspicuous.
An Admirable Aim—In Need of Proof
None of this is to suggest that the initiative is without merit. On the contrary, it is admirable—indeed, exemplary—that the MHRA now seeks to engage patients, stakeholders, and the broader public in the co-production of medicines information. One can only hope that this commendable commitment extends not merely to the refinement of language and format, but to the substantive inclusion of material that has, in earlier iterations of regulatory communication, proven somewhat elusive.
Conclusion: Transparency in Practice
In short, transparency is a most splendid objective. Its true test, however, lies not in its declaration, but in its application—particularly when the information in question is awkward, contested, or inconvenient.
One awaits, with interest, the practical demonstration of this newly discovered virtue.
AI Whisperer
The RxISK Team fortunately has a gifted AI Whisperer – able to prompt AI systems to come up with imagery that has tranformed a set of just loaded videos into something much more loaded than they would otherwise have been. It’s worth enjoying these and getting a sense about what can be done that would have been impossible a year ago.
- Isotretinoin and Consent
- Finasteride and Consent
- Bad Trips on SSRIs
- No Sex – We’re on Antidepressants
There are two more gems in the series to come.
- Good Trips on SSRIs
- Consenting to SSRIs
Update
There is a great set of comments below which involve an interaction between Anon – a critic of AI Slop – and Ron who is defending what you can do with it.
Ron’s evidence lies in a 42 – page Chat GPT document linked here – its a much quicker read that you’d expect from 42 pages.
So thoroughly nice of you to give us a good laugh. We do like the slow, drawling lilt of a master talking about the Loony Tunes
Conclusion: Transparency in Practice
In short, transparency is a most splendid objective. Its true test, however, lies not in its declaration, but in its application—particularly when the information in question is awkward, contested, or inconvenient.
One awaits, with interest, the practical demonstration of this newly discovered virtue.
MHRA are so thoroughly upright, uptight, crocheting with their needles, wearing their pearls, at the weekly club to discuss their stitches. It’s all Tic-A-Dee-Boo adjusting their furniture to fit their expanding duties. You can never have enough bureaucrats popping their ‘we must care for the people’. ‘Hey, that’s a good idea’.
Decades ago when I asked my doctor if she had sent in a yellow-card about me and Paroxetine, she was so shifty, she ummed and ahhed so much, I thought I had better do it myself. I felt very self-conscious sending in my little report to the Nation’s Important Regulator. The reply was gobsmackingly uncreative. Full of gobbledygook and impertinent in a life-changing and deadly situation.
Woodnewton
Figure 17: Example of an instruction leaflet for flatpack furniture – P.65 of 80 – The Billy
I have a ‘Billy’ Ikea bookcase in my caravan
Woodnewton – guess the ‘wood’ went to their heads – Silly Billies
Well done on the ‘gems’. ..
This is an anonymous comment
This deep state post is pretty good. I have lately been experimenting by asking various AI sites to show me the case for the involvement of Zoloft in mass murders, suicides, and homicides. The persistence of AI slop is undeniable.
Also, I tackled these questions with using Grok, an AI bot, on questions of the role of Zoloft in mass murders and the role of SSRIs in PSSD. Here is what got spit out:
There is no definitive, exact number of mass murderers (or mass shooters) who were specifically on Zoloft (sertraline, an SSRI antidepressant) at the time of their attacks, because comprehensive, verified databases do not track this detail uniformly across all cases, and much of the available information comes from media reports, court records, or partial investigations that are often incomplete or unconfirmed.
Reliable, peer-reviewed studies and large databases (such as the Columbia University Mass Murder Database) show that antidepressant use—including Zoloft or other SSRIs—is not common among mass shooters and does not exceed rates in the general population.
Then I said, what about the effects of SSRIs in people under 25 in terms of sexual dysfunction. Again, this is what it spit out:
There is no precise, well-established rate of persistent sexual dysfunction (known as Post-SSRI Sexual Dysfunction or PSSD) specifically in young people up to age 25 after taking SSRIs such as paroxetine (Paxil), fluoxetine (Prozac), or sertraline (Zoloft). Large-scale, controlled epidemiological studies focused on this age group do not exist, and systematic reviews conclude that reliable prevalence estimates cannot be determined due to underreporting, selection bias in surveys/case reports, lack of standardized diagnostic criteria, and confounding factors (e.g., depression itself can affect sexuality).
My conclusion? Whatever I produce on any question I know anything about is going to be verified by some kid in a researchers or politicians office armed with Chat GPT and he’ll conclude I’m a moron that doesn’t know what I’m talking about because what I am saying is so inconsistent with the AI expertise. Deep state indeed.
Is there a way to get around this ?
In the case of the Grok response on Sex I think its citing an article of mine – pointing to the exact difficulties some of us cited in getting reliability — but the article also says the problem we the authors thinl this problem is undeniably real and perhaps common.
The get around can’t depend on accidentally realizing Grok is citing me. The get around also needs to get around the fact that journals now have screens in place that will reject articles on PSSD or any new hazard of meds – perhaps on the basis that there is no prior literature – but if the screens keep rejecting submissions on this basis there will never be any prior literature.
In the last two days, I’ve had three different people have articles on adverse events rejected without review. They got almost instant replies – which strongly suggests to me algorithmic screens in place.
We need an Ariadne to lay down some thread to get us out of this AInotaurs labyrinth.
David
Ron has responded to Anon above
I started this with the initial question… the role of Zoloft in mass murders and the role of SSRIs in PSSD.
I just played with some risk related issues… The problem Anon raises is if the regulator/responder doesn’t know the subject and just gets AI to write a response… without critical thinking or expert peer review… IMHO AI needs and expert moderator/peer review.
Thoughts?
DH – Ron sent a 42 page ChatGPT printout – which Ive linked into a note at the bottom of the main post above
I am quite sure ‘anonymous’ above is not a moron.
My view would be to play this at their own game. Publish newspaper articles, with verified facts and figures, without focusing too much on AI. I think newspapers, radio interviews, podcasts, have a much wider intelligent audience, than AI ‘spits out’. Also, legal cases, and much has been published about those in Medical Journals and elsewhere.
Look at the case of a possible retraction of Study 329.
A lawsuit against the American Academy of Child & Adolescent Psychiatry and its publisher, Elsevier, demands the retraction of a 2001 article in the Journal of the American Academy of Child & Adolescent Psychiatry (JAACAP) – Study 329, completed in 1998 and funded by GSK, revealed serious safety risks — including suicidal behavior — associated with Paxil. Later studies confirmed those risks.
Most sensible people know that AI Slop in the murky world of Adverse Effects, Suicide, Homicide and violent acts, are very real dangers, and AI Slop cannot disprove that.
Instead of continually reaching out to AI, powerful voices are needed in the media and beyond, and that is not beyond most peoples’ capabilities. Especially from serious Academics.
Remember the article in the National Post, Canada’s Press, about Tumbler Ridge and an Inquiry. This lady journalist had some power in her hands.
Maybe to beat AI, a better use of Journalism might be in order to activate against AI Slop.
Ron’s 42-pager –
5. Bottom line
Zoloft/SSRIs and mass murder: no convincing causal evidence; at most, a rare contributory role via behavioural activation in vulnerable individuals.
SSRIs and PSSD: a legitimate and increasingly acknowledged risk, with a consistent clinical pattern and growing regulatory acceptance, though mechanisms and prevalence remain incompletely defined.
Thoughts? Yes, Ron.
Annie
There is a problem here. Not only do medical and academic journals not take articles on adverse effects any more, the lay medial – from the so called best like the BBC to the NYT etc stopped 15 years ago doing so in the interests of Fair Balance. If controlled trials have shown a drug works and is free of side effects it is not Fair to give an airing to problems that maybe don’t really exist or are caused by the illness being treatend and in so doing to put people off getting treated. The media – lay and academic – are told you will have blood on your hands.
You seem to think it is simple. I can see nothing that you or Anon or Ron have offered that can make much difference. At best we can have some fun Fiddling while Rome burns.
D
.
‘Britain’s medicines regulator is MHRA, who you could say are the Still Heart of a Beating UK Healthcare World – just to be clear Hearts are still when dead. But in their afterlife, bureaucrats will continue to seem to do something as a cover for doing nothing.’
This – and Ron’s sustained fugue in haute ironie – made me laugh.
Ron has elevated the MHRA’s quest for ‘meeting information needs’ to his own intellectual and ethical level. Having scampered through the WoodNewton Research, it is clear that this is a quest not for transparency and integrity of content, but for lucidity of communication style. Surprise, surprise – patients want to see larger font sizes, summaries of key usage and ‘side effect’ information upfront, more graphics etc. Basically to make the fly spotted loo paper of current PIL design into a contemporary user friendly piece of communication.
The brief was effectively for an information usage behaviour (known as ‘the journey’ in marketing circles – a term that makes me squirm for reasons I can’t pinpoint) and comprehension study – a very basic type of research. With such a large sample, there would have been an opportunity to do something more enlightening – contextualise the findings by segmenting the sample into different information user mindsets/psychographics – but that was too interesting and not in the brief.
I hunted for insights. Nothing much there really. A few jangly notes – there was a high degree of trust in the ‘leaflet, in part because it was recognised as legal bottom covering by industry.
“Don’t write it in a way that is blatantly obvious the manufacturer is protecting themselves from future litigation”.
At the same time as trusting the PIL, there was dare one say a healthy suspicion of AI bespoke slop.
‘The way in which AI could HALLUCINATE and provide very misleading results, particularly where the AI designed to ‘satisfy’ the user. This would become more of a risk, the more AI was used to personalise guidance on medicines, for example on contra-indications or the effects of taking multiple medicine.’
I can’t believe this was as widespread as the report suggested – but who knows?
Ron’s ChatGPT demo – and debates I’ve had with Grok – show that AI can talk as much sense as we can think. Applying the principles of geoengineering risk to drugs is not just Ron-smart, it’s sensible. To name but a few elements, ‘building in uncertainty, stratifying risk by severity (not prevalence nonsense), non-disclosure represents a breach of duty, not a neutral omission, failure to adequately communicate risk leads to secondary harms generated by the system itself’ Yes, yes, yes, yes. ‘Suppressing hazard information is not a recognised safety strategy in any comparable field’. Exactly.
It’s a tight and reassuring blueprint. But how can we implement it – and how can we implement it when so much of the data is still ghostly garbage?
This is a great comment – on the ‘journey’ we are facing grappling with all this.
The algorithms dump almost all comments from you – including this one – into Spam, sometimes without even telling me they have gone in there – so it will be the luck of the draw if I have a twitchy instinct and check out which becomes harder to do if yours is mixed in with 50 others and not possible if its with 300 others
Of course your instinct will be to attribute some perverse vendetta to me – rather than building a resisting community we will be fractured
D
Go the extra MILE
Responses to enquiries to drug companies by Health Care Professionals are increasingly being automated.
Explore https://www.mile-association.org/current-publications/
The key is SRDs: Scientific Response Documents
Fiddling while Rome burns –
This story is rumbling a lot in the Press; most media picked it up and drew with it. Most grieving parents will want answers, but are they missing the elephant in the room and why should they suspect ‘medications’ that the shooter admitted to when ‘medications’ are the last thing on people’s minds. RCMP nonchalance, it’s ok to have guns in the home.
Tom Kingston was drawn to a gun in his toxic drug state.
Family of child injured in Canada school shooting sues OpenAI
https://www.bbc.co.uk/news/articles/c309y25prnlo
In an open letter to Canadian officials on 26 February, penned by OpenAI’s vice-president of global policy and shared with media outlets, the company said it had implemented a series of changes in recent months, including enlisting the help of “mental health and behavioural experts” to assess cases and making the criteria for referral to police “more flexible”.
RCMP, on the alert after Tumbler Ridge, have arrested two boys in Nova Scotia and Manitoba, with the FBI and Interpol involved, in a possible school shooting planning.
Canada is facing a crisis, but what is the crisis?