Editorial Note: This post merges the Go Figure sequence of posts from several weeks ago with the 329 series.
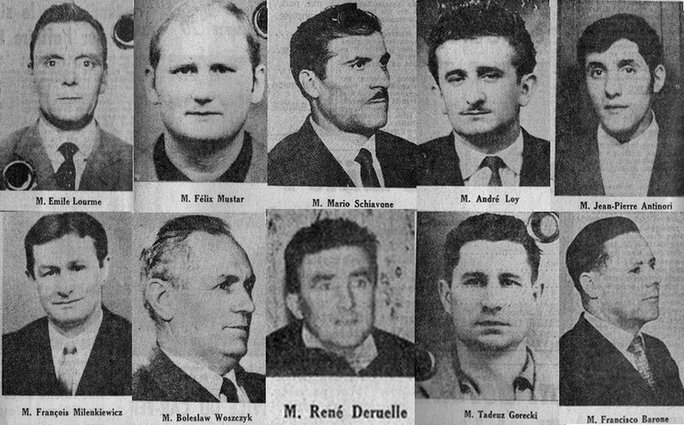
In the wake of the French Revolution of 1968, the government was still tottering when on February 4 1970, sixteen miners died with twelve others maimed in an explosion at a mine in Lens in France. The mine owners pitched the event as an accident. It didn’t help their case that Northern France had a history mine disasters, including the worst ever in Europe in 1906 at almost exactly the same spot, when over a thousand men lost their life. This is the reason we have insurance, the owners said. This is what the law of 1898 was all about.
The miners called on the Left-Wing philosopher Jean-Paul Sartre to prosecute their case. Sartre claimed there were no accidents, the owners knew there would be a certain number of deaths each year and factored this into their costs. There had been five the year before in a nearby mine. While injured workers thought of their job as risky and that when injured they had just been unlucky, they were wrong. It was murder, Sartre said.
Calling these deaths murder made the disaster an event. If it was murder, the owners should go on trial. Capitalists in general should go on trial. Perhaps even the government. This was a pivotal moment for the Left. Despite the lack of trust of many in France in their government, society didn’t follow Sartre down this route. Perhaps because the French State made a display of solidarity. The Left lost its grip to a New Left and others who were looking for a Third Way.

A century earlier faced with a predictable number of deaths from anesthesia each year, American surgeons in the first place, because anesthesia was developed there, faced questions about the ethics of doing evil in order to do good. If the patient died from the anesthetic, were they murderers?
We somehow collectively decided that no they weren’t. No-one sees us as duped for doing so, even though roughly one per thousand anesthetic events today lead to death. There are likely more deaths from anesthesia than from mining disasters each year. There are certainly more deaths per person year exposure.

The death of the comedian, Joan Rivers, some years ago under light anesthesia for an endoscopy, rather than plastic surgery, threw a light on this issue. Deaths under anesthesia have been happening for one hundred and seventy years but every so often a death or other happening becomes an Event. In this case, nothing happened.
“With plastic surgery, the general anesthetic is like a black-velvety sleep, and that’s what death is – without waking up to someone clapping and going, ‘Joan, wake up, it’s all over and you’re looking pretty’.
What is less forgivable perhaps is that anesthetists have a blind spot for the difficulties that may emerge days or weeks later linked to their procedures and agents.

Where do the adolescents or young adults or any of us who commit suicide or homicide triggered by an SSRI taken, or given, on the back of studies like 329 fit? What do we call this?
British papers over the weekend were full of a trial involving a footballer and an inebriated woman where he was convicted of rape in the first instance, with the sentence later quashed in controversial fashion. American and world media were filled with stories of Donald Trump and the question of consent. In the light of Study 329, is the consent people or their families have given to take a medication like paroxetine any more valid than a consent that after the event an inebriated woman is claimed to have given?
Like the mining accident in Lens, the Evans rape trials, the Trump candidacy, the republication of Study 329 is an event, possibly a pivotal moment. Details outlining trends in the rate at which articles are ghostwritten, or patients enter hospital because of treatment induced injuries are features of the contemporary landscape but every so often these features come together to make an Event and Events make history. They create a before and after – even if not necessarily right there and then.
“Whaaat do we call this?”
I have thought about this for a long, long time.
The nearly killed me, covering their tracks, most unprofessionally..
You can’t call it murder……you could call it Medical Negligence, you could call it Medical Homicide by Default, you could call it Passing the Buck and you could call it Undercover Reporting.
GBH and DH……..
Whatever, you call it, GlaxoSmithKline did nothing to stop our UK Doctors Dishing It Out and that may be Murder..Ask Sir Andrew Witty what he thinks..
“the republication of Study 329 is an event, possibly a pivotal – even if not necessarily right there and then.
Perfect!
Whoa, lots of big questions here! A few points that strike me:
In the case of coal mining & similar hazardous industries, everyone enjoys the benefit but only a (marginalized and devalued) minority take the really big risks. Even if workers feel they have no choice, they know they’re being treated as disposable commodities … risking their lives for the benefit of others who take no risk. The question of Murder is NEVER too far from the surface.
With medications, it’s a somewhat different story. They are always said to be prescribed “for our own good.” The benefits to millions are said to be worth the catastrophes that befall a few thousand — but also, those who benefit and those who take the risk are allegedly the same people. We’re given a similar narrative about air and auto travel. We usually accept this if we feel the following things are true:
1) The technology saves far, far more lives than it costs — either by curing deadly/crippling diseases or by ending a lot of poverty and backbreaking labor.
2) The captains of industry and/or govt are doing everything they can, within reason, to minimize the risks. Sheer negligence in the service of profit is not being tolerated.
3) We are being informed honestly of the risks so we can exercise at least some limited forms of choice. For instance we can choose to live with a disability rather than take the risks of surgery, or we can forego driving when the roads are slick with snow or we’ve been drinking.
4) Everyone is more-or-less equally exposed to the risk. The poor aren’t asked to endure a more regimented and risky form of healthcare than the wealthy.
When it comes to SSRI’s and other psychotropic drugs, are any of these conditions being met? I’d say NO on all four counts. What do others think?
It is certainly true to say that the republication of Study 329 should be seen as a ‘pivotal moment’ but, for this to be so, surely we need to see a dramatic change in attitudes towards the inaccuracies of the first Study 329, as well as to the revelations in the ‘Restored’ version, by those in power? I feel that they are extremely slow in their condemnation of the original and also in their praise of the restored version.
Talking to any member of the general public about ‘hidden information’ etc., one is often met with dismay – however, I’m not sure it goes beyond that. For the ‘pivotal moment’ to become a reality, we should hope for a dramatic change in patients’ questioning of suggested prescriptions as well as far more suspicion amongst doctors concerning the reliability of pharmaceutical information, coupled with a firm stance from parliament showing that such dubious standards of patient care will be no longer be tolerated in this country. Then, and only then, I feel, can we hope to see a massive difference in the ‘mental state’ of our nation resulting in NHS care for ALL at the point of need – but tailored to the individual need rather than a massive ‘force feeding’ of many whose main need may well be a supportive hand to help them on through an emotional period in their life.
Victoria Derbyshire (Used to be on Loose woman) is covering withdrawal this Wednesday on her show “Victoria Derbyshire” BBC 2 0900-11.00.
From Surviving antidepressants:
ikam
Gold star
Members
PipPipPipPip
1,060 posts
Locationuk
Posted 16 October 2016 – 05:33 AM
Petition update:
A very exciting development!
from James Moore
Caldicot, United Kingdom
15 Oct 2016 — I have some exciting (and slightly terrifying!) news. The Victoria Derbyshire show is shortly going to run an item looking at the experiences that people have taking antidepressants, including the difficulties some users have when attempting to stop. As part of this, all being well, I will have a short live interview about this petition.
This is such a great opportunity to gain some much needed awareness of the struggles that so many have using these drugs. If you can find the time please watch and, even better, contact the show to share your experiences. We need to demonstrate how many are suffering in silence, unable to get the help they need, this will make a huge difference and a real impact. Let’s light up their Twitter feed like a Christmas tree!
The broadcast details are:
– The Victoria Derbyshire show
– BBC 2 and BBC news channel
– Wednesday 19 October
– 0900 to 1100 BST
Contact details:
– Twitter: @VictoriaLIVE
– Facebook: http://www.facebook….toriaDerbyshire
– Email: victoria@bbc.co.uk
– SMS: 61124
– WhatsApp: 07753 428 430
Thanks so much for all the support.
Here’s another one from Surviving Antidepressants for anyone who wants to get involved:
LesleyAshmall
Getting started
Members
Pip
1 posts
LocationLondon
Posted 04 October 2016 – 07:07 AM
I’m a British BBC TV reporter and I want to make a film about the problems of withdrawing from antidepressants. I’m keen to hear from people who’ve struggled with SSRIs, particularly if you like in the UK. Also what you think about the lack of support groups, or if you HAVE a support group, how do you help?
Please email me your stories, confidentially at first, of course, although ultimately I’m looking for people who will be willing to stand up and speak about what’s happened to them. I think few people know or report this sort of problem and I know many of you are really really struggling for help. My BBC2 programme wants to expose all this, so please get in touch.
Lesley.ashmall@bbc.co.uk
Thank you very much. This forum has been recommended to me by several long-term members, so forgive my intrusion.
CORPORATE HOMICIDE?
‘The extreme side effects of antidepressants’ – http://www.bbc.co.uk/news/health-37682355
They can always find someone, can’t they?
“The drugs companies have declined to comment, but Dr Sarah Jarvis…” (will repeat ad nauseum all of the usual s***e about how safe and effective these drugs are).
Walter
Considering that, like a programme on any topic, Victoria Derbyshire’s programme had to ensure there was no bias shown to either side of the argument, I feel that, overall, the outcome was definitely an acceptance that adverse reactions EXIST and can be EXTREME and that problems on withdrawal are REAL and sometimes impossible to overcome, resulting in an impossible withdrawal task. That, to me, is a huge step in the right direction. I think that introducing the report in sections was an excellent opportunity to ‘catch’ different sections of society e.g. – parents back from school run, shift workers returning from work, people in witing rooms, pensioners settling in to their morning’s viewing( !)etc.
The daily cost to the NHS of antidepressant prescriptions should be enough to shake awake the most lethargic viewer surely. It is catastrophic! People can argue till the cows come home about ‘benefits versus harm of ADs’ – seeing that daily total in £s on the screen should unite all to the idea that a thorough investigation into the whole business is long overdue.
Let’s hope that there will be coverage too of the ‘presentation’ to Jeremy Hunt on the news later today. When will the Panorama programme air I wonder? Hopefully soon whilst this morning’s revelations are fresh in the mind.
The complete BBC Victoria Derbyshire segment is online — and wonder of wonders, it’s actually viewable in the USA!
http://www.bbc.co.uk/programmes/p04ch68x
Very good all in all …
Spot on Walter – very well said – ’tis s***e indeed ! And VERY irresponsible, ignorant s***e at that.
Is Sarah Jarvis not aware of RxISK and all it’s very informative content? Obviously not – how is it that I, a mere mortal, know LOADS more about akathisia than the vast majority of GPs and, worst still, the vast majority of psychiatrists who, as consultants and therefore supposed ‘specialists’ in their field, surely should have a compulsory duty to keep up to date with all the significant research and therefore able to recognise a clear case of akathisia when it’s staring them in the face – but they can not and will not – ignorant in the extreme and totally shocking (to a mere mortal like me)
I think the biggest problem we have here is to do with ‘perception of harm’. One person’s words can be perceived differently by every single listener. It is impossible to compare people’s suffering without actually witnessing the person’s state. Many doctors barely lift their eyes towards the patient – they are glued to the screen in front of them and fingers are poised for a prescription. Taking these facts into consideration, it is no wonder that Dr. Sarah Jarvis was so reluctant in her acceptance of withdrawal problems. I do think that Victoria Derbyshire should have asked her how she would deal with the ‘vulnerable patient’ suffering, years down the line, ‘from their own vulnerabilities and not from the tablets’. We know the answer – more medication then further medications to settle the reactions to their initial prescription. It would have been interesting to see how she’d have got out of that one!
I sympathise quite sincerely with all of you who feel disappointed with the programme – in the main, that will be because you have, or still are, going through the mill of withdrawal. You all listened and recognised every single symptom that was described. I have witnessed many of the symptoms therefore I can visualise from the descriptions. The general public will hear the words but, unless they have suffered in this way or have witnessed the suffering, they CANNOT possibly visualise what you have all gone through. Words alone cannot take us near to the suffering that you have all endured. Your torment doesn’t come near to anything else that I have ever witnessed in my life. One young woman described the seizures that she suffered – I witnessed similar occurrences which I had described as ‘an epileptic fit without the frothing’ therefore, once she spoke those words yesterday, I could picture exactly how she’d suffered. Had I not witnessed it, my picture of her suffering would have been a very weak impression of the reality of her situation.
It is because of these difficulties of visualising others’ suffering that I was so delighted (in a horrified way!) to see the annual AD total for England and the daily cost to the NHS shown so clearly on screen. Those two facts, in my opinion, will have registered with people watching the programme yesterday or later online. It is a sad fact of life that most will probably find it easier to be horrified by those facts than by the descriptions – vivid as they were to us – given by sufferers.
Maybe it would be easier to convince the general public of the horrors of psychotropic drugs by using facts such as these and David’s ‘1 in every 4 has some difficulties…..etc.’. To me, the most important point is to RAISE AWARENESS of the horrors – in whichever way catches the imagination. Once hooked and listening, there would then be a better chance of their appreciating the true depths of your suffering – and how you were ‘wronged’ by so many who should have known better, also how you need the acceptance that it was the tablets, not you, that were faulty – and, in turn, companies coming out and declaring such so that you could at least have the peace of mind that you had, at last, really been believed by all layers of society.
It would appear not Jane.
Sarah Jarvis stated:-
“With some severe depressions you may need to try two, or possibly three (SSRIs) before you find the one that does work”.
Isn’t this a particularly powerful way to produce AKATHISIA in those who are vulnerable to this dreadful and often unrecognised neurotoxicity?
The associated changes in behaviour, personality, the induced suicidality and risk of violence to self or others is then misinterpreted as a “First Episode Psychosis’, leading to the process of psychiatric
mis-management and sequalae so eloquently described by Katinka Newman.
Sarah Jarvis went on to observe: –
“What we have to bear in mind is that some people who have taken these have been very very vulnerable. They’ve been very anxious and it can be very difficult to tell what is anxiety and what is the tablets”.
There are clearly very difficult issues for primary care physicians here.
Surely however, not recognising and correctly diagnosing “barn door obvious” akathisia is inexcusable?
More subtle, perhaps gradually emerging akathisia presentations may indeed be challenging diagnostically.
Akathisia should be the first consideration in differential diagnosis in those given SSRI’s who re-present with sudden catastrophic deterioration.
Those who never had a depressive condition, for example “stress” – “exam nerves” must usually be easier to accurately diagnose than those who presented in severe depression?
Akathisia must first be explained, and information given carefully and accurately by the prescriber each and every time an SSRI or SNRI prescription is written.
SSRI induced sexual dysfunction.
Bravely introduced by a respondent. Again an ADR poorly understood by prescribers.
It seemed a bizarre coincidence to listen to The World Tonight on BBC Radio Four later that day. (approx. 10-25 pm).
Emeritus Professor of Forensic Psychiatry, Don Grubin was interviewed regarding his suggested use of SSRI’s as an alternative to “chemical castration” in self volunteering sexual offenders.
This appeared to be a powerful endorsement as to the potentially devastating lowering of libido (et al) induced by SSRIs.
Sincere thanks to those who presented accurately with wisdom, sincerity and powerful experience.
ABSOLUTELY “Akathisia should be the first consideration in differential diagnosis in those given SSRI’s who re-present with sudden catastrophic deterioration”
SO, why isn’t it? And how does this get rectified? How are our medical ‘professionals’ to be trained, re-educated about the crucial need to include Akathisia in their ‘check list’ and for it to become the ‘number one tick box’ in the diagnosing process?
And how are the new generation of current and future medical students to be educated properly about this?
The BMA (and similar professional organisations) MUST be held to account – they are key to making this happen but it seems they just won’t listen (believe me, I’ve tried!)
‘Answers on a post card, please’
Timothy Moss hits the nail (or, wish it was) the GP on the head. Sarah Jarvis is never going to ‘get it’ is she?
‘Getting the right pill for the right patient’ sounds so comforting and almost exciting. A magic potion awaits you if the sorcerer just composes the perfect spell. If not, it’s back into the cauldron with you, little frog, until she finds something else to dose you with. And if, after all her hocus pocus and weaving of spells, you are much worse and end your life, well, there you go then, one less frog to worry about. Onto the next.
All anxious and depressed little frogs, we must find a safe, warm welcoming ponds for you, covered with hospitable lily pads where you can rest, talk out your worries, and stop the world for a while. How can we do this, because do this we must. We can’t wait for the sorcerers to wake up and see reality. They are lost in their spells and their hubris.
Well put, Heather – my thoughts earlier today were exactly: ‘there’s witches* at work!’
Endorsed 100% when I received an email circulating which said:
“Dr Sarah Jarvis has received honoraria for lecturing, chairing meetings and attending advisory boards for Astra Zeneca, Janssen, MSD, Novartis, Sanofiand Takeda”
http://www.issuesandanswers.org/wp-content/uploads/Novartis-PCCJ-symposium-showfile_FINAL.pdf
*actually not really cos ‘witch’ is too much of a compliment as most witches were, in fact, very wise women and not greedy for BigPharma payouts!
The Corporate Manslaughter and Corporate Homicide Act 2007 is a landmark in law.
http://www.hse.gov.uk/corpmanslaughter/
http://www.hse.gov.uk/corpmanslaughter/about.htm
Prosecutions will be of the corporate body and not individuals, but the liability of directors, board members or other individuals under health and safety law or general criminal law, will be unaffected. And the corporate body itself and individuals can still be prosecuted for separate health and safety offences.
Companies and organisations should keep their health and safety management systems under review, in particular, the way in which their activities are managed and organised by senior management.
https://en.wikipedia.org/wiki/Corporate_manslaughter
Identification doctrine
This approach holds that the offence of corporate manslaughter is made out when an individual commits all the elements of the offence of manslaughter and that person is sufficiently senior
to be seen as the controlling mind of the corporation.
Timothy and Annie – yes, corporate manslaughter on a vast scale. To clarify – it can’t be murder as murder requires a direct intention to kill (exemplified by Shipman) not simply egregious indifference as to how many people might die or be severely injured.
Problem: as Annie says, the principle that a company can commit criminal manslaughter was established back in the 1970s, a bit tortuously, by deeming directors to be the equivalent of a brain. But, sad fact is – there have to my knowledge been virtually no successful cases. Maybe because the analogy of a vast corporation being similar to a human being falls flat on its face when it comes to the immensely complicated notion of what on earth constitutes the required mental/intentional bit of manslaughter…if you are bored enough to google ‘manslaughter’ and ‘mens rea’ you will see just how complicated it it – and why so many law students fail that bit of the exam.
Yes, to answer David Healy’s question – ethically, morally and by every decent human standard – murder. Legally? No way.
So – we have to find another way of holding people to account. Changing the prevailing attitudes to ADs, all medicines, doctors, research, mental illness etc etc. I think Study 329 was absolutely pivotal in pushing that change forward.
Grrrrrrrzzzzzz…………………………?
Victorious?
Doctor “surprised if it related to tablets”
Still not listening; the ‘doctors’
I have never been struck with depression, I do not do suicide, I swallowed Seroxat
Brilliant patient responses and brilliant David Healy responses
All we need now is a Prog Ram completely dedicated to Seroxat/Paxil containing all the Corruption, the original 329 authors, the China Syndrome, the $$$3 Billion fine,, the recent win by Breggin – as he swallowed a T shirt….the International Court Cases with Tobin, Stewart Dolin, David Carmichael, etc. etc. etc.
There are UK Litigants, waiting in the wings
David Healy is an Expert Witness in Courts of Law, with the legally defining data and evidence
For this, we are extremely grateful
Well done Katinka, James and David……….you three looked and sounded all very lovely. 🙂
No SSRI’s were named
ANTI-DEPRESSANT DRUG SEROXAT
Session: 2002-03
http://www.parliament.ukedm/2002-03/1203
Could you also add Citalopram, Prozac, Venlafaxine, Sertraline,escitalopram,fluvoxamine and any others not mentioned to the list too. Thanks.
BBC News NI: Pregabalin/ Lyrica: Home Office urged to make prescription drug a class C substance
http://www.bbc.co.uk/news/uk-northern-ireland-37574709
On the matter of consent: if you, as a patient, recieves bogus and frauded information on your pill, then ‘consent’ has not been given. Simple as that.
The mountain of difficulties I have climbed in order to get a more truthful view of what Seroxat really is, just shows that no one can call it consent in the first place.
My doctor is still living in “1999”, clinging to that Seroxat is safe, and, “that all pharmaceuticals have side-effects”.
And as long as I listen to my doctor, nothing has changed since 1999.
If I listen to David Healy, my life gets an obvious explanation. But not even DH can change the minds of the swedish psychiatrists. Why would they change their minds and agree they have abused, without consent, the minds of hundreds of thousands?
Ove2016
“We still going to call it consensual?”
https://www.madinamerica.com/2016/10/go-figure-study-329/
Early day motion 1203
ANTI-DEPRESSANT DRUG SEROXAT
Session: 2002-03
Date tabled: 13.05.2003
Primary sponsor: Gidley, Sandra
Sponsors:
That this House calls for the anti-depressant drug Seroxat to be withdrawn from use for new prescribing pending an urgent, fully independent review of its and other SSRI anti-depressants’ safety, because of the extensive evidence of severe withdrawal reactions and an increased risk of suicide associated with it; and calls on the Medicines and Healthcare Products Regulation Agency in conducting the review to include people with experience of using Seroxat and to make full use of the consumer-based evidence and research available, such as that conducted by Panorama and Mind.
http://www.parliament.uk/edm/2002-03/1203
Disquiet..
“transparency theatre”
http://www.aftenposten.no/meninger/debatt/Unpublished-trials-are-a-cancer-at-the-core-of-evidence-based-medicine–Ben-Goldacre-607061b.html
http://www.alltrials.net/
Robert Frost
GlaxoSmithKline..3.44
http://www.alltrials.net/find-out-more/why-this-matters/
Discord..
Andrew Garratt @andrewcwgarratt
It’s a good campaign but I see on #AllTrials features of party political ones (and I’ve run a few!): spin, hype, misdirection.
https://twitter.com/statsguyuk/status/789118490733060096 …
Adam Jacobs @statsguyuk
Since my comment on the latest #alltrials video still hasn’t made it past the moderation queue, here it is again
https://twitter.com/statsguyuk/status/789118490733060096
ben goldacre @bengoldacre 1h
ben goldacre Retweeted forskning.no
I’m having an argument with a Norwegian Minister about whether he should let publicly funded researchers withhold trial results #alltrials
http://forskning.no/helse-forskningsetikk-forskningen-du-ikke-far-se-om-forskning/2016/10/kunnskapsdepartementet-kjoper
– I get a bad feeling of his proposals, said Mr Bjørn Haugstad.
https://translate.google.com/translate?sl=auto&tl=en&js=y&prev=_t&hl=en&ie=UTF-8&u=http%3A%2F%2Fforskning.no%2Fhelse-forskningsetikk-forskningen-du-ikke-far-se-om-forskning%2F2016%2F10%2Fkunnskapsdepartementet-kjoper&edit-text=
Go Forskning.no
What struck me almost straight away when I was struck with Seroxat was how the narrative changed straight away.
Straight away it was accusatory from doctors who grasped me like a nettle and spun their spin.
From the instant referral to the mental hospital psychiatrist, without telling me, from the Indian doctor who started this whole ball rolling..
From the “are you suicidal?” almost the first words uttered from the psychiatrist sitting in my stunning lochside abode which I had spent fourteen years ‘doing up’ and was the sort of place he wouldn’t own in his dreams/lifetime of drugging up people in his mental hospital.
Verbally attacked by the gp for two years, three years, until I transferred.
All those posters you now see in doctors waiting rooms and hospitals ‘Abuse towards Staff will not be Tolerated’
I would charge that there is more abuse directed towards patients on ssris and benzos and antipsychotics than any other situation.
The amount of verbal abuse I withstood was second to none.
Culminating in the most outlandish, with the most affront at decency, telephone call from Canada, which was a deliberate act of profound bullying of a patient..
Their story as written in my medical records ignored all drugs, ignored the mother and child alone, completely trashed an air ambulance pilot and to a lesser degree my own mother, and, yet, this sort of twisted behaviour was allowed..
It is akin to the doctors surrounding ‘the patient’ with a lasso and dragging the wretched thing along a dirt road at 100mph as she twisted and turned and gave up a flurry of dust specks and was so invisible as a human being that it could be a carcass
And, for this to happen in an idyllic scottish countryside setting and not in one of Cormac McCarthy’s books; well, I am lucky I am well-read..
http://quarterlyconversation.com/cormac-mccarthy-essay-the-orchard-keeper
GO F:
The Fall-Out:
https://www.facebook.com/david.healy.7773
https://www.facebook.com/FiddamanBlog/?fref=ts
Katinka Blackford Newman
20 October at 20:10 ·
Yesterday I appeared on the Victoria Derbyshire programme on antidepressants. It was a great opportunity for the issue of people being harmed by side effects to be aired. However there were, in my view, some factual inaccuracies which I have complained to the BBC about. This is the link to complain to if you agree and want to make your own individual complaint.
http://www.bbc.co.uk/faqs/complaints_process
So here was my complaint.
…
On 19 October the Victoria Derbyshire Show aired a programme on antidepressants . In the programme commentary there were two factual inaccuracies. There was a statement that depression is caused by low serotonin which antidepressants can rectify. There is no scientific basis for this claim and indeed some antidepressants lower serotonin. Even mainstream psychiatry reject this: Sir Simon Wessely, President of the Royal Psychiatrists has said “Most researchers have long since moved on from the ol serotonin model”.
It was also claimed that for the majority of people, antidepressants are beneficial. There is no scientific research which backs this up. Antidepressants are tested only for a short term (maximum 12 weeks) by the drug manufacturers . There are no studies – either short term or long term that show that more people benefit than are harmed. If anything, the data supports the opposite, which is that over 50% of people who go on antidepressants stop taking them within a month because of side effects. Therefore it cannot be the case that more people benefit than are harmed. The BBC represented this not as a view, but as a fact. The fact is clearly incorrect and therefore the BBC is not upholding standards of accuracy and impartiality.
Julia Schopick Presents Honest Medicine shared David Healy’s post.
19 October at 13:56 ·
Thanks to Katinka Blackford Newman for sharing Dr. David Healy’s post. Dr. Healy has been warning people about the dangers of antidepressants for many years. From the article accompanying this video:”People who say their lives have been ruined by commonly prescribed antidepressants, known as SSRIs, are taking their case to Parliament on Wednesday. Some users say the tablets have made them suicidal.” Katinka’s book tells her personal story about how antidepressants almost ruined her life
https://www.facebook.com/profile.php?id=100011691003465&hc_ref=SEARCH&fref=nf
dr david corbet @corbetron
he shouldn’t. #nobrainer #transparency #alltrials
https://twitter.com/bengoldacre/status/789459481449070592 …
ben goldacre @bengoldacre Oct 21
ben goldacre Retweeted forskning.no
I’m having an argument with a Norwegian Minister…
He shouldn’t..
http://www.the-scientist.com/?articles.view/articleNo/47323/title/European-Drug-Regulator-Releases-Clinical-Trial-Data/#.WAtNMuN36Ak.twitter
http://www.fiercebiotech.com/cro/alltrials-welcomes-ema-s-transparency-drive-as-it-posts-first-set-csrs
#he shouldn’t
Take All the Praise……………Bad Science..
https://www.facebook.com/whocaresinsweden/?hc_ref=NEWSFEED&fref=nf
whocaresinsweden.com
3 hrs ·
Känner du någon som tar eller tänker börja ta SSRI, antidepressiva medel? Se denna film för att vara medveten om vissa biverkningar som kan förekomma.
https://twitter.com/DrDavidHealy
Today11:00
BBC Radio 5 live
In Short..
http://www.bbc.co.uk/programmes/p04crc87
The doctors’ union, the British Medical Association is calling for the urgent introduction of a 24-hour helpline for patients who get addicted to prescription drugs.
5 live Investigates has found that some people have been prescribed powerful drugs – known as benzos – for decades, although guidelines say the maximum should be four weeks.
The BMA will say more specialist services are needed for people who have become addicted to drugs prescribed by their doctors. As well as a dedicated helpline, the organisation wants clearer guidance for doctors on how to help people cut down and stop taking prescription drugs.
Jan Waterton fought her addiction to Benzos for 18 years and suffered severe side effects
This recording is originally from 5 live Investigates on 23 October 2016.
Release date:
22 October 2016
Prescription Drug Addiction
http://www.bbc.co.uk/programmes/b07zxrdb
Jane has given us a very interesting link, see her comment on Oct 21st responding to my ‘frog and sorcerer’ analogy, in response to Timothy Moss earlier. She points out that Dr Sarah Jarvis has received honoraria from several drug companies. Nothing wrong with that, one might say, but it begs the question, are there really no ordinary GPs, unattached to drug companies, in the whole of London (or anywhere in the UK) that the BBC could have found to give an unbiased view? And, shouldn’t it have been made clear that she had these links, so the audience knew?
Also, the psychiatrist Dr Linda Gask, brought in for the opposing view to DH, had coincidentally recently written a book, which I had coincidentally just read, and on which I’ve commented elsewhere on these Blogs. She had oodles of psychoanalysis and therapy before she took anti-deps herself. Years of it. She was more iffy about them in the book than she was on the programme. She started feeling low after her father died, due to unresolved family relationship issues, (fairly common I would have thought) but by the end of the book, many years later seems to feel she has a serious mental illness…it’s a well written candid read, very honest about her feelings.
I used the term ‘sorcerer’ not ‘witch’ because, like Jane says, there were some wonderful old Wise Woman ladies who got labelled as witches, indeed I think I may have been one in a former life……a bog standard one, I hasten to add. I just ITCH to find a solution to this ghastly Catch 22 situation we find ourselves in, fighting to be believed, fighting to protect, to save life. Hey ho, Hallowe’en is soon upon us, let’s get our pointy hats on folks and see what we can do. Because, sure as eggs is eggs, we’ve got to find a way to change things, we and others, for years and years, have talked it round and round in circles, maybe we need some magic now.
Heather
What if anyone affected asked upfront “Do you not believe me?” and refused to engage further without an answer? If the answer is No I don’t believe you, then it is clear you have to go elsewhere.
David
David
I apologise if I am being very stupid but I don’t think I understand what your comment here actually means? Could you, or anyone else who ‘gets it’ explain it to me? 🙂
Heather
Heather, I’m pretty sure that my reply is miles off David’s actual meaning – but here’s what I made of it! If you, as a patient or carer, are dissatisfied with the treatment that is given – when you describe the reactions you have suffered or seen – and fail to engage the professionals with the realities of your suffering (showing that they do not believe you) then you have no choice but to search for another professional willing and able to treat you. Not being believed, or listened to, is the end of the road – nothing further can be gained from that relationship. ‘Treatment’ relies on trust from both sides. Once that trust is broken, no improvement is possible. I suppose that I read it this way because it is true of our situation in the past.
Thanks Mary. I was relating it to my comments on the Victoria Derbyshire programme, but your way I see it in a wider context.
Round and round, the GP Circle…
Listen to this:
http://www.bbc.co.uk/programmes/b07zxrdb#play
Podcast up shortly
If GPs don’t listen to you, then it is clear that you have to talk beyond the Grave..
Too little, too late; your GP holds your life in their balance..
The Council for Evidence-based Psychiatry
39 mins ·
The BBC has today broadcast a programme on BBC 5 Live which reports on the BMA’s call for a 24 hour national prescription drug helpline. Dr Andrew Green, the BMA’s GP clinical and prescribing policy lead, told the programme: “Establishing a national helpline should be a top priority to provide better service to individuals with prescribed drug dependence. “There is also the need for specialist services to be consistently available across the country.” [ 81 more words ]
http://cepuk.org/…/dr-james-davies-bbc-250000-long-term-be…/
http://cepuk.org/2016/10/23/dr-james-davies-bbc-250000-long-term-benzodiazepine-users/
Better to
Die on your Feet
than
Live on your Knees
UCLA/ISEPP – David Healy
Mad in America Video
https://madinamerica.com/
“you’ve got to shout and keep shouting”
Thank you
Dear DH. Annie, and others,
I was being a bit flip about sorcery, and in apologise.
David Healy says ‘ if people don’t believe you you have to go elsewhere’. And Annie quotes. ‘Better to die on your feet than to live on your knees’. Another contributor on the Blogs wrote recently about it being a good thing that Hitler was not behind the dilemma we find ourselves in. DH once mentioned hunger strike in a post, but I think you’d get labelled anorexic and find yourself being stuffed with medication. I think he was kidding anyway…
It IS a dilemma because I think we’d all agree that what is happening to people badly affected by these medications are having their lives permanently or at least temporarily stolen and in many cases ruined. And we are having enormous difficulty in being believed, unless we, or a loved one, has suffered, died, had their previously normal lives totally changed for the far far worse. So it is like a war, with lots of nice well meaning henchmen carrying out policies which are doing terrible harm.
So the moral dilemma here is that, for those who really do feel they gain benefit from these drugs, be it placebo based or whatever we do not want to take away their rights to have them. But we have a Duty of Care to warn everyone, then it’s their choice. And we do need to find better safer treatments for all, and to get some energy put into this, which won’t happen as things are, when the problems are not being officially dealt with effectively.
In 1940, just before Dunkirk, things were looking pretty grim for us in our efforts to fend off Hitler’s dastardly plans. So in May, the King asked that all who felt comfortable with it, on a chosen National Day, should ask the Almighty for a hand…. Now, times have changed and organised religion is not the bit thing it was then, but lots of us do know about Energy, the Universe, the power of goodness, angels etc, whatever floats your boat. In 1940. The weather changed in our favour, and the sea became calm just right for the British boats to get safely through. Now, that could be coincidence of course. But who really knows? The point is something worked that made all the difference to our fight for freedom.
I know this is going to sound off the wall, and I don’t suppose for a moment that this kind of ‘going elsewhere’ is what DH meant in his response to me, but a lot of us do believe in the power of good over evil. I have read lots of books about Energy, including one called ‘The Field’ which explains the energy force of the Universe and how combined thoughts have a great effect.
On November 2nd it is All Souls’ Day. All round the world, people remember their departed loved ones, and there are some quite interesting ceremonies enacted in many different countries. This is not about witchcraft, it’s about love and respect. How would it be if as many of us that can, and feel comfortable in so doing, light a candle at 9.00 pm that day, (BST) and send our positive thoughts into the Universe, asking that we be helped in the furtherance of our cause, to protect all those who are being, or who have been, or in the future may be damaged by these medications, and for us to really be taken seriously and properly assisted by those in power, in the near future to right this terrible ongoing wrong. In other words, to make sure all are listened to, and that tremendous care is taken before mind altering medications are ever prescribed. That immediate and consistent monitoring takes place. The drug companies, like Hitler, seem to hold all the cards right now. We are only asking for goodness, honesty and decency to win, over greed and subterfuge. If it worked to help us defeat Hitler in 1940. why don’t we try this, all together, just this once? What have we got to lose? I shall do it, whatever.
I shall be amazed if this gets past the Moderator, but what the heck 🙂
Heather, you have brought tears to my eyes with your comment this time. I feel your sense of urgency and your dedication to the plight of so many coupled with your fear for the many more who will be swallowed up by this immense greed that surrounds us all.
I would like to add to your comment, on the line of ‘things otherworldly’, that Christianity was a very slow-moving, poorly understood and hardly believed (to put it mildly!) when the message to ‘spread the word’ was first put forward all that time ago. Now, whether one believes in the Bible or not, it cannot be disputed that Christianity eventually took a hold and became a power for goodness. (Before anyone jumps in with the ‘more wars caused by Christianity…..etc’. – may I just say that we can always find another side to every coin if that is our wish). To me, the ‘power of goodness’ is exactly what keeps you going Heather and I commend your idea of ‘the power of prayer’. However, one prayer in earnest has a greater possibility of being answered than a thousand in mock reverence – but a power beyond our understanding is a real possibility and the results can be astounding. On a personal note – when our son was in a coma, his sister ( who hasn’t attended church since her Sunday School days) put a message on Facebook explaining the situation and asking all to pray for her brother that night. His plight was also included in our minister’s prayers the next morning. We had already been warned that getting our son out of the coma unscathed was highly unlikely – but, when we phoned the ICU for an update on his condition at lunchtime, we were told that he had miraculously woken from the coma and seemed to be responding. Make of that what you will – whether it was the prayers or not, I shall be eternally grateful for whatever powers were at work on that Saturday night through to the Sunday lunchtime.
There are also powers that we do understand – movements that are visible to us all – and I feel that things are on the move regarding the prescribing of strong drugs. Looking back to 2002, when we, as a family, first became aware of these drugs, I would say that there is more belief in the dangers of these medications now than there was then. Sure it’s very slow-moving and we’d all like to see a swift awakening to the realities as we see them but that is not the way that these things happen is it? If we can keep moving forwards then, eventually, our goal will be within sight. We need to keep positive and not become downhearted – nor down-trodden. We should keep on giving anyone that we meet the information and the choice of joining us in standing up against the evil caused by these drugs to so many. However, we must also bear in mind those ‘others’ who seem to benefit from the very same concoctions. We must raise awareness – we cannot demand compliance. Our way of dealing with this issue should always show our compassion towards those who suffer and our hunger for a firm belief that all is far from good in the pharma camp.
Heather, I’m in.
That’s great Laurie, thank you!
Mary, I’m a great believer in miraculous recoveries and hope, and the power of good things happening. That’s so wonderful about your son’s experience, coming out of the coma. One is always anxious not to thrust one’s beliefs onto others, trying at all times to remain credible to the skeptics whose views of course are equally valid and reasonable. But I’ve experienced a miracle myself when all hope was lost, and once you’ve been there, you long to wear the tee shirt and tell the world :).
Listening to the piece Annie found for us on Radio 5 Live yesterday made me feel that, just like you say Mary, things are turning the corner at last and gathering momentum. It was about people badly affected by benzodiazepines, Valium etc. The presenter said their phone lines were overwhelmed, they’d never run a topic with such a massive and unprecedented response.
Hooray!
I think Annie must have been Sherlock Holmes in a previous life. I think her sleuthing is fantastic. She must have radar up on top of that caravan. Big Pharma don’t have a chance, with her on their case. Thanks so much Annie for your wonderful research. 🙂
Yes!!! – at last parliament has realised that the cost of all this ‘medicating’ is actually in £££££s as well as lives! The APP Group looking at drug dependence have decided to support the BMA’s call for a helpline etc. as well as commenting on the cost of remaining on medications due to withdrawal problems etc. Every day ( since the V Derbyshire programme) TV news have brought us new snippets to do with mental health medications. 5 Live Investigates was also a very influential addition I thought. The response, as you say, was astonishing. I think the day is drawing near when every doctor in the land will realise that it’s time to come out of the shadows and stand tall for the rights of all patients.
As for Annie, well, what can I say! – where would we be without her? Annie, I sincerely hope that the time you spend researching is as therapeutic for you as your results are for us. I hadn’t noticed the Seroxat mug by the way – the Costa product placement was the one that caught my eye! I watched again and did see the mug that you mentioned – right next to the ‘Keep calm’ mug. David – I hope that you’re not suggesting a link between keeping calm and taking Seroxat!! Maybe that’s why Costa was there too – as your alternative for a calm outlook on life!
Heather,
Your concept is very powerful and although I have no religious commitment we feel compelled to prepare our candle.
The concept of a silent vigil, augmented in spirituality as a candle-light presentation of our shared overwhelming grief is comforting just to imagine.
For all those devastated, destroyed, conventionally bereaved;
for all those enduring an indefinite bereavement with a living-whilst-dreadfully damaged loved-one, such a visible and tangible shared statement might provide more than a dignified yet immensely powerful message of hope and determination.
Such a vigil could state that prescription psychotropic drug poisoning is a reality that cannot be further denied.
A reality that cannot and will not be tolerated.
Let these candles “speak” to those doctors we trusted but became doctors whose non-consented casual prescriptions maimed, destroyed and killed our loved ones.
Just maybe, such a vision might begin to make them question their appalling and arrogant false beliefs in SSRI safety and efficacy.
During such a vigil, attended by those who truly understand the almost indescribable iatrogenic suffering caused by SSRIs (in those vulnerable to their devastating ADRs) – we may be able to provide spiritually for each other.
Perhaps it might be possible to create that support, empathy, understanding and compassion so palpably absent from the appalling experiences of “professional” – “Ignorance Based Care”.
To those who have been made to endure SSRI/SNRI induced akathisia, suicidality, violence against self or others and then the personal and family catastrophe of false diagnosis of S.M.I. with incarceration with institutionalised brutality, – we may provide some small measure of comfort.
How extra-ordinarily powerful to choose All Souls Day.
It is the souls of our destroyed loved ones, and the souls of those of us who strive to care for them –
(without any formal rehabilitation, or other support or caring services)
It is these souls that have been stolen by these fraudulently licensed and often enforced psychotropic drugs.
Sorry, we’ll be out of British Summer Time by the 1st and 2nd of November. I would think if we sent off positive thoughts across those 2 days with lit candles in the evenings, we can work across continents with time changes.
Timothy, what a wonderful response, which says it all, to perfection. Yes, let’s stand together and support each other spiritually with our candles, lit for all those who suffered and died, and all those who suffer a living hell from the effects of psychotropic drugs.
I should maybe add, (as I feel I am amongst friends here). that November 2nd has very special significance for me and Olly’s dad. It is the day 4 years ago that Olly’s ashes were taken by us to a final resting place. I remember feeling, somewhat strangely, as I carried the little wooden box to our car, (wrapped in his favourite blue hoodie sweatshirt so passersby in the street outside the Undertakers’ wouldn’t realise what was in my arms), that it weighed as much as he used to when he was carried in my arms when very small. I thought to myself, how can we be doing this, when the last time I saw him, two days before he died, he said ‘give me a hug Mum’ and stood by his front door, his terrible pain so obvious in his sad eyes, wearing the same sweatshirt. How could this be real? I couldn’t believe that his (and our) trust in doctors and their potions, and worst of all, their misjudgement of this lovely, thoughtful, beloved young person who we’d known for 32 years, could have resulted in this awful moment, and the only tangible evidence left was what I was now carrying along the street.
I am sorry if this memory is too personal, but it shows graphically the end result of what we are all tirelessly fighting to stop. The senseless loss of human life, and the appalling devastation being caused to those who take the medication and somehow have to live with shattered minds. Those whose only mistake was to trust others, who were doctors and drug manufacturers who had seemingly no idea about, nor care for the consequences of their actions.
On a happier note, like Leonnie has said, when she writes of her son, I know Olly has gone nowhere. I know he’s OK. Well, much more than OK. A little voice in my head said the other day, “suggest to them they light candles and stand together, Mum. It could work, don’t worry what anyone thinks, just say it”. So I did, and those who feel the same can all send off our wishes together, in hope and solidarity, with more REAL power than any drug makers or inept prescribers, simply because our cause is just, and in the end, good always overcomes evil
Heather,
We find your post “for Olly” to be the most moving and powerful testimony. Thank you.
Yes, most moving and powerful – thank you for sharing, Heather.
I have recently discovered numerous Facebook groups who are all discussing much the same thing as we do here on DH’s blog in their various different threads and I wonder if you would like your wonderful candle concept to be spread further and wider through these Facebook groups?
I would like to help spread the idea so please do let me know if I can help.
Oh yes please Jane; I am just finalising plans with Katinka as to the best way to do this, and will be writing something on our Olly Friendship Foundation facebook page on Tuesday 1st November about how so many of us want to each light our own candle on Wednesday 2nd November at 9pm.
Then on that same Facebook page we’ll put our own candles on on the night of the vigil, on Wednesday 2nd at 9pm. If you have a look on that page you’ll see we’ve used Olly’s tree like this before, but for Easter eggs to remember all our lost RoAccutane youngsters, and we also have named lanterns for them which we light on the anniversaries of their passing. We have little glass votives for candles on their birthdays. We also write a bit about Olly, in the hope that it comforts his friends, and also in the hope that we can appeal to others to hold onto life whilst we try to find solutions to this dreadful Big Pharma problem. Also to empower them to ask questions before they take mind altering prescribed medication.
I’ll write more when Katinka has added her ideas. I don’t have Twitter but I think she does and can maybe do that too. It would be nice if people sent their candle picture and message somewhere if they want to, so we can see them. More to follow…..
Heather,
I’m in touch with Katinka (and we’ve met on a few occasions) – I’ll email/tweet her and no doubt she’ll forward my contact details to you – so we can get the ball (or rather the candles) rolling ….. such a wonderful idea …… I’m sure many will gain solace from lighting a candle and knowing that they are sharing this with other like minded folks far and wide.
Jane and everyone interested in showing solidarity with the “candle’ initiative. Your enthusiasm is wonderful, thank you!
I suggest we liaise through emailing Katinka.
You will need a picture of a loved one, either sadly lost, or still suffering on, or with remaining damage from prescribed drugs having stopped taking them or struggling with withdrawal symptoms.
Light a candle beside their picture and think of them with love and positive thoughts at 9 pm on Wednesday 2nd November. If you can take a photo of them next to their candle, (making sure that you have the permission of the person if they are still living) our idea is to then post it on Facebook, or, if you are not connected to Facebook, but can email it to Katinka, she will put it there for you. (Find her by Googling – Katinka Newman -The Pill that Steals Lives)
Of course, you can even send a photo of yourself by your lit candle if you feel solidarity with all of us who are trying to show how much we need help to overcome the terrible problems BigPharma is causing us by producing drugs which are doing so much harm to many people. We are not trying to stop choice, so of course medications should still be available for those who want and need them, but they must be made honestly aware of all the risks before they take them. And most importantly of all, AKATHISIA must be recognised quickly by all prescribers and their relatives, and appropriate action taken.
We are also wishing with our powerful thoughts together on All Souls’ Night, for safer and more compassionate treatments to be found, so that a lot of the risks can become a thing of the past. And most of all, we are asking, in solidarity, beside our lit candles, to be listened to and believed by doctors, the public, the media, and all those who have control of medical policy.
Heather, would you be okay with me sharing the following? Also, I’m just wanting to double check, is 9 PM your time 5 PM eastern time in the US?
Post:
On November 2nd, All Souls’ Day is observed all around the world. People remember their departed loved ones and there are some quite interesting ceremonies enacted in many different countries.
Heather Roberts, who lost her son in 2012 to his prescribed medications, has suggested that those of us concerned about pharmaceutical harms might observe All Souls Day by lighting a candle and sending positive thoughts out into the Universe…
…for the protection of all who have been, who are being, or who may in the future be, damaged by prescribed medications;
…for all persons now affected, that they be listened to, taken seriously, and properly assisted;
…for tremendous care to be taken when medications are prescribed, and for immediate and consistent monitoring;
…for this ongoing wrong to be righted, now and in the future.
Because the drug companies seem to hold all the cards, she has suggested we ask the Universe (or God) for a shift, so that goodness, honesty and decency might prevail. May we do this out of love and respect for all who have suffered — both living and departed.
For more information please visit Olly’s Friendship Foundation page on facebook.
Laurie, this is perfect, it says it all, exactly as we need it said. Thank you so much for doing this.
As to time changes, our British clocks have just gone back, so you are 4 hours behind us. So 9pm here is 5 pm with you, like you said.
You could also refer people to Katinka’s website, as she is sending information around and receiving it, particularly with the Candle Vigil.
On our Olly’s Friendship Foundation Facebook and website we have information on the medications that affected Olly, in particular RoAccutane/isotretinoin and Seroxat. We also try to make a difference in helping anyone who is feeling desperate like Olly was, to try to give them hope, and encourage them to hold on. We describe what happened to him and say a bit about his life. In a way, it keeps his memory alive for us and his many friends who were so shocked by his death and miss him so much.
Katinka is more in the centre of things, and has more people linking in with her who have suffered from ADRs.
Thank you so much Timothy. We’ve felt so alone with all this for the last 4 years, fighting for some recognition of how he suffered and how he was wronged. He was truly a really lovely guy. Now we feel we have found a place where others like you understand and are trying to save others. That’s what he wanted.
https://www.theguardian.com/education/2016/oct/27/patients-must-understand-options-royal-college-surgeons
RE Johanna’s 3rd point – we can only consent to any form of treatment if we have all the information – plus all the risks – and where psychotropics are concerned that is simply a great big blank. But…this link is about a Court of Appeal decision last year which opened the door a chink to the start of Informed Consent in the UK. Previously – we had no such legal doctrine to rely on – you simply signed a form before an op to say it was OK to go ahead on the basis of virtually no actual info about how likely you were to die or be damaged. With drugs – absolutely no legal obligation for a doc to discuss side effects – or to really give you a choice as to what you wanted to do. (If you did try and have that conversation, as everyone on this blog knows to their cost, you were immediately dumped in the ‘trouble-maker’ trash can).
The article is good and worth a read. I’d assumed that when the Court of Appeal decided that the woman in question (who’d brought the claim) had a good case for compensation, no real precedent would actually have been established. Why? Because when a decision has huge implications for medicine, potential litigation and costs to the national purse it will usually be restricted to (similar) cases which are likely to be rare.
Now – the Supreme Court has decided, 7 judges, a unanimous decision – that the principle that all treatment requires a full disclosure of all the risks and has established the right of the patient to make their own choice. It’s a massive leap forward. Nothing will change anytime soon as old habits die hard but it does open the door for all patients to sue if the principles of really informed consent to treatment, set out by the judges, aren’t followed. Sadly, no good to any of us as decisions can’t be applied retrospectively but might just make a big difference for future victims.
Sorry to be a bit legalistic – read the article for all the details – but as medicine will not regulate itself, Big Pharma continues to utilise every possible, disgusting way round its dishonest and immoral marketing practices – then being able, at long last, to use the law is a gigantic step.
This is fantastic Sally. Like you say, a great step forward! Your legalistic input is brilliant, don’t apologise for it, the Guardian article you link is really great, thank you!
Just to add – re Davids’ last point – yes, things come together – not just the Supreme Court decision, but questions and discussion about flagrant abuse in all areas – rape, racism, Trump, the list goes on. Victoria Derbyshire’s program got aired, Katinka’s book, this reporter interested in interviewing people withdrawing from ADs. There just seems to me right now a sniff of a sea change around a lot of things – medication included. RIAT’s Study 329 WAS a vital pivotal moment in my view – for all the reasons I stated in my blast of irritation, the original ‘Go Figure’ post..
The Berlin Wall came down in a astonishingly quick time eventually – much sooner than I’d expected. The build up was slow but in the end it was torn down in a week or so. Big change can happen – rumblings can morph into an Event.
Absolutely agree Sally about the sea change and things speeding up.
Heard on the News today also that doctors are being advised to ask patients to discuss and jointly confer with them on all the various options before deciding on treatments (including drugs to be prescribed) and so avoid being sued (!)
We need to keep the pressure on, if we feel we could be on a roll at last.
Back to the Drawing Board
If, in the interests of science, when adverse effects are discovered then it could be an opportunity to ask what is happening to these patients when others seem to benefit? If there is genuine openness and a will to delve much deeper into the workings of the mind, then these adverse results could provide a window to study and and see the causes.
Instead of recrimination, perhaps researchers could share expertise and develop new tools and a greater understanding of the factors at work. I think, it is a pity to discard, what might have been genuine and constructive thinking, because of adverse results. This information may be useful and some of it still valid.
I think, the competition and profit ethos may have to be realigned.It may be necessary to rethink their way of working and approach in order to fulfill their true responsibilities to humanity and long term scientific and ethical requirements. There is still much to achieve and we must not compromise our our intelligence and conscience!
Barry Broadmeadow
Barry, don’t you think a State Pharma Research Institute, with no profit connexion, is maybe what could work – reading your last paragraph. Then an honest ethos, concentrating purely on understanding what treatments REALLY work for the good of those using them could hold sway. I think for some industries, nationalisation works. Not many, but for pharmaceuticals, definitely.
As to the ‘workings of the mind’, we do seem to be getting back to basics better on this. Today on BBC One Breakfast programme, Norman Lamb (Lib Dem MP with responsibility for their Health policy) was interviewed with his son Archie, who has had mental health issues and at one point wanted to end his life. The theme of the discussion was getting fathers to talk, from an early age, with their sons, about things like anxiety. Sharing feelings. I think minds would work a lot better later on if we listened and talked honestly and sensitively with our children and friends from an early age, with no fear of recriminations. This would surely be ‘constructive thinking’ at its best?
Heather,
Thanks-I am very worried about the way politicians and society seem to continually “put the cart before the horse” and many skilled psychologists are aware of the many of the causes of mental illness and also how they could be avoided altogether. Prevention is better than cure and in many walks of life steps could be taken to help each other to avoid cruel processes being inflicted, for quite unnecessary motives.
The family setting may be the most fertile ground for learning how to reduce children’s problems and enhance development. Parenting classes can bring about a transformation in children and, of course, the once beleaguered parents. Also behavioral therapists could turn around the lives of troubled kids.
Unfortunately, there are long delays and hence children are given pills instead which is usually counterproductive. Health Managers don’t seem to grasp that it is cheaper to prevent children being put into the adult system in the first place. The escalating cost of adult care and the inability to cope with mental illness is not going to be solved with wonder drugs but they haven’t twigged that they need to spend on education and prevention. If we don’t invest in the appropriate care for each other the problems will deepen.
Under too many burdens and unnecessary demands individuals and families snap and so far we just leave it to the doctors to deal with it. There needs to be a different way of approaching health issues and not by ignoring the blatantly obvious. To avoid devastating and costly consequences for all concerned people need to be honest about our behaviour and the need to change it. This sadly runs throughout our society but with a genuine will this could be changed.
I’ve worked as a children’s author illustrator invited into schools to do Workshops over the past 30 years. What I’ve noticed particularly in the last decade is that the children seem to have become much more materialistic and also judgemental about appearance. Incredible cruelty can be inflicted on anyone, child or adult, by shunning them and pronouncing them ‘ugly’, or to use current slang, ‘a minger’. I am almost certain that a lot of the self harming and desperate unhappiness amongst the young, is due to them being obsessed with having to look acceptable, and being IN the group, not excluded from it.
Olly, our son who died in 2012 had bad acne and was rejected by ‘the lads’ at school because of it. He was sensible and an entrepreneur, but the deep hurt of being thought ugly, and often taunted about this in public, laid down a learnt insecurity. It was the acne drug and Seroxat which took away his remaining resiliance. But to pick up on your point, yes, good parenting etc will doubtless help, but society’s whole attitude towards selfishness, materialism, short term ism and profit before everything, rubs off on the young. It’s like osmosis, they get it almost by default, from everything they see and hear around them. We need kindness extolled as the top virtue, not how good we look on ‘Strictly Come Dancing’. Like you say, it’s no good expecting doctors to pick up the bits and pull rabbits out of hats to magically introduce happiness. Children need quality time doing things together in families, sharing fun, being listened to, appreciating simple things like nature, that are free. But parents live pressured lives and it takes special effort and thought to build this in. It pays dividends in the end though if those children can avoid psychotropic and acne drugs.
The ‘All Souls’ Night’ Candle Vigil is going really well, we are standing together for the reasons Laurie Oakley has listed so brilliantly on this string, and we have echoed them on the Olly’s Friendship Foundation facebook page. Pictures of candles and wonderful supportive messages are appearing one after another.
We really do need to get our points across. This morning we attended an NHS Seminar for service providers on the new Wellbeing Hub system, the first point of entry for GPs. Carers, patients etc, to access mental health services. We asked if we might speak for a few moments about our aims in relation to raising awareness of all Dr David Healy said on the Victoria Derbyshire BBC2 programme, ‘Anti-depressants, Curse or Cure’ (19.10.16 at 9.00am). We held up a huge sign showing the word AKATHISIA and asked people to raise their hands if they knew what it was. In a hall full of well over 50 NHS and other service providers, not one person had ever heard of it!! So we enlightened them and signposted them to our site for more detail, using takeaway handouts, also mentioning Katinka’s book ‘The Pill that Steals Lives’ and site, and Robert Whittaker’s ‘The Anatomy of an Epidemic’. We received lots of interested support, and many of them said they had learnt something very important this morning and will follow up. So, onward and upwards, and may our collective thinking and solidarity push on for good change!
There was another audible intake of my breath when I read the brilliant news about your raising of the AKATHISIA “flag” at the NHS Wellbeing Hub Seminar.
The previous gasp was listening to Sarah Jarvis.
No surprise that none had heard of akathisia. I wonder how many of these newly informed providers are regular SSRI prescribers?
No surprise that many, perhaps most, prescribers are not able to recognise, diagnose and effectively and safely manage acute SSRI induced akathisia.
If the word is unknown, they can have no awareness of the most serious and dangerous adverse drug reaction which is commonly caused by one of their most widely prescribed classes of drugs.
No surprise that they mis-diagnose akathisia as “agitated depression”.
Change to another SSRI or increase the dose of the current drug and aggravate the intensity of akathisia and its intense iatrogenic suffering.
No surprise then – that now, completely out of their depth, they refer to (apparently) equally ill-informed psychiatrists who rapidly label and libel as
“Psychotic Depression”. —
Psychiatrists who (apparently) do not immediately prepare a careful prescription drug history in order to identify the correct and clearly identifiable cause of what may have now become a toxic psychosis.
They appear to have forgotten how to differentiate this acute medical/neurological emergency from a functional psychosis.
The guideline treatment for the latter is a medical catastrophe for the former.
The catastrophe could also be avoided by listening to their patient, or if the akathisia is too intense, listening to family desperately trying to convince these doctors that this is so obviously due to the drugs.
One of my most admired physicians of the early twentieth century is the Canadian, Sir William Osler: –
“Listen to the patient, they are telling you the diagnosis”.
Heather, your achievements at this seminar are another EVENT. A brilliant demonstration of how to get our point across.
(We have a photo of our candle and symbols of our stolen “soul”.
Do you have an direct e-mail link please)?
Tim.
Tim, I think most of those attending the NHS WellBeing Hub seminar were those in NHS posts tasked with signposting sufferers to get help, service providers working for Local Authorities, Housing Associations, MIND, counsellers from Hospices, HealthWatch, and so on. I think they were all non medical. They say they find it hard to get GPs to engage with the idea of using Wellbeing alternatives.
The new big thing now is to have a central WellBeing Hub for Mental Health in NHS Trusts,, (with, wait for it, just 3 people taking telephone referrals, one or two of these part timers) for self referrals or GP referrals, to get mental health support for anyone requesting it as primary care. Those of us who have been NHS Stakeholders in the Trusts for about 5 years and attended countless of these meetings, tend to mutter cynically between ourselves that this re-arrangement of deck chairs on the NHS Titanic is really just about a way of cutting frontline costs. However, it did strike me that if we can get our information across to all these agencies like we did on Wednesday, and they can offer this knowledge, whilst at the same time offering their signposting to self help groups and welcoming Day Centres, it may avoid some of the anti-depressant etc prescribing, for those only moderately depressed or anxious
.
So it might just be a GOOD THING in a funny sort of way…..
We asked how long it would take for someone, having rung in and referred themselves or a patient, to get psychological therapy. Answer – said with some degree of apology – about 6 months. So no change there then! You are on a list. A box can be ticked somewhere. But in the meantime, they would offer them/you these other groups to join, to get the company of people like themselves, walking groups, gardening, swimming, reading self help books etc.
Also on offer are courses like Moodmasters, Mental Health First Aid, Mindfulness etc, and some are free. Once logged in, having been signposted, the WellBeing Hub staff do not feel the need to follow up in any way. We all felt this was very poor and protested in unison.
BUT, if at gatherings like this we can spread the word about AKATHISIA and as parents of someone who has died by prescripticide, shock them into realising the horrendous reality of what this means to us personally, then maybe they can be useful. We have to admit that till we saw Josh’s film on Katinka Blackford Newman’s ‘The Pill that Steals Lives’ Blog, we didn’t realise why Olly had so often had to battle those kind of endless movements. We were told by psychiatrist and social worker and PSN it was attention-seeking behaviour, acute anxiety, and to ignore it. We realise now it was the lack of being able to stop, sleep, think, which made him finally, in exhaustion, and unbelieved, give up the ghost. He said in his last days ‘I am just SO tired, please let me go, and forgive me.’ No wonder…
Tim, in answer about email contact, you can write Visitor Posts on the Olly’s Friendship Foundation facebook page, or you will find, on the website which precedes our helpline number. Leave a message if not answered at once, and give your contact details, email etc and we will email you back. Also, to post a picture of your candle and message, put it onto the Facebbok page where you’ll find several put there by other supporters, with comments. We are all standing together in solidarity, so, definitely the more the merrier, thank you!
I should add, that they assured us that if someone self referred by phone and listening to them they ‘sort of felt it was a more serious immediate problem ‘, they have access to patients’ Care Notes, to see if they are already ‘in the system’, or they can go along the corridor to consult with people more au fait with acute problems, and presumably they would bring in the Crisis Team if those people made the judgment that it was appropriate. But the Wellbeing Hub phone answerers are the gate keepers, and one does worry as to how much clinical understanding they have.
It’s all so difficult to grasp, new changes and systems coming in all the time.
In the end, people who are ill with anxiety or depression want timely one-to-one support, a person face to face to speak to, to see a way forward, as soon as possible. They do not want a telephone conversation about where they might go and then be left alone to either take up the suggestion or not, with no follow up. They may be in such a state of terror they can hardly pick up the phone to make the call in the first place. They need someone to take them along to wherever it is that they are meant to get help. And their families/ those looking after them 24/7, if they are lucky enough to have them, need support and advice too. Along the lines of ‘Open Dialogue’. If only……
forgot to say..Peer Support Workers are being trained, so if we have lots and lots of them, maybe they can act as understanding buddies. But we are going to need enormous numbers of them, with very good training, and if they’ve been ill themselves, they need a lot of support too to make sure the strain doesn’t wear them down. Perhaps cutting the drugs bill could fun an army of well trained understanding people.
Thank you for your comprehensive additional information.
I have learned great deal.
Tim.
Heather, thanks for these very interesting posts …… An ‘Akathisia flag/banner’ – Wonderful!!
Yes, “The System’ sure is complex!
I do like the idea of Peer Support Workers ….. presumably these are voluntary? And, of course, very good training (particularly about Akathasia) is crucial.
But ‘understanding buddies’ can be a ‘God send’ …… no one can understand like someone who has ‘been there, done that’ and recovered/come to terms with it all…… or, very sadly, had to live with the consequences.
Is this NHS Well Being Hub a local or national initiative, I wonder? And which particular policy is the driving force? If we could ‘get to’ the strategic lead person in charge, maybe we could influence the content of future training programmes.
I’m very interested to learn more ……
Jane, The WellBeing Hub seems to be unique, so far, to our county, but no doubt, with the single market they will be selling it as an idea to other Trusts, as this seems to be a good money spinner. They like to sell initiatives to each other.
Peer support workers are ex- patients who are trained to come back and help other in- patients. But some say, seeing others on the medication regime that made them themselves feel so ill, and seeing that the prescribing policy doesn’t change, it takes a big toll on them, they want to save others from the damage they’ve experienced. Buddies sound a better idea, they don’t have to have been on the wards I think. They too may have experienced mental health poisoning. Often they will have managed to get their lives back on track, so they are inspirational. We were told years ago they were being brought in, but there hasn’t been much sign of it.
We went, with our AKATHISIA banner, to a NHS Locality Form today, attended by about 20 others, some admin, some Trust stakeholders, some carers, many working in Mental Health. NOT ONE of them had ever heard of akathisia! I can’t honestly say they expressed much alert interest either. Our little speech went down like a lead balloon, very different to its reception at the Well Being Hub Seminar, interestingly. Then later they were bemoaning the lack of money in the NHS leading to a service that had forced them to cut corners. We pointed out that each day the NHS spends £780,000 on psychotropic drugs. ‘can’t we recommend savings there, being mindful of the additional damage these drugs do for many who take them?’ A further embarrassed silence ensued. Then ‘ah, but we can’t question the prescribing habits of clinicians’ ( in other words, the unaccountable god-like beings). No, maybe not we said, (wondering why on earth no one has the guts to do so?) but you can watch out for and quickly report akathisia, and you can raise awareness, write to your MP, Dept of Health, pass the word wherever you go. More embarrassed silence. Anyway, on we go, and undaunted. But so far, in a week, we have learnt that 70 or more NHS people have never heard of akathisia, so there is much work to do!
The GMC are currently revising their advice to medical practitioners on consent.
Perhaps they need to have sight of your brilliant AKATHISIA banner.
With regard to the response: – “ah, but we can’t question the prescribing habits of doctors”
Why ever not? – except of course that within psychiatry any patient or relative questioning a prescription places themselves at risk of ridicule, retribution or even an arbitrary increase in dosage as punishment.
The GMC states (to their registered medical practitioners) –
“You must protect patients from the risks of harm posed by colleagues prescribing, administration and other errors”.
“You should question any decision or action that you consider might be unsafe”.
Might it not be argued that patients and relatives, as well as doctors, have a DUTY to question prescribing habits?
“In a week, we have learned that 70 or more NHS people have never heard of AKATHISIA”.
Time indeed for some intense questioning of a profoundly dangerous lack of awareness.
Sorry to report that yesterday, a month after the NHS Forum event, we attended another, and were given the Minutes of the previous meeting. Very disappointed not to find the word AKATHISIA there, after my 5 minute effort to explain the urgent need to get it understood, to save lives. There was only a sentence just stating that a member of the Forum had expressed concern about the overprescribing of medicines. The whole point of AKATHISIA had been missed. When I queried this, I was shocked to hear the Chairman say I had hijacked ‘their’ meeting and should not have raised this! The Community Engagement officer added that AKATHISIA is an anacronym ( in other words, initials representing something ) and people don’t like these. It was evident that no one had bothered to research it further, and did not want it reported in the published Minutes. It struck us as extraordinary. Surely the point of such NHS stakeholders’ Forums is first and foremost to raise awareness of dangers to patients; my information was offered in good faith in ‘any other business’. I was therefore very surprised to hear this critical tirade from the Chairman yesterday. It will not shut us up, however, it just makes us all the more determined to shout AKATHISIA from the rooftops…:)
Tim, I’m sad to say, our experience in 2014/2015 in putting Olly’s case to the GMC, describing in accurate detail the appalling behaviour of the Lead Home Treatment psychiatrist, was more than disappointing. Having first consulted a young psychiatrist friend, who ran our Letter of Complaint before her own Professor of Psychiatry, we felt we were in with a good chance of being understood and supported, having made all the amendations he’d suggested. Especially since Olly’s tormentor had been up before them before due to mistakes on his watch leading to suicide, reported by another psychiatrist colleague.
It is true that when telling Olly how Olanzapine could ‘change’ him, that man had described it well. What he seemed unable or unprepared to grasp, was the fact that Olly was suffering Akathisia from this man’s instructions to stop Venlafaxine immediately, without tailing off, and with no regard to the fact that prior to that, he’d been on Escilatopram for over a year. He’d also been on Zopiclone to help him sleep, the akathisia having surged when doses were changed. Olly’s anxiety, restlessness, feeling of terror, started to overtake him, with the endless suicidal thoughts, when the Venlafaxine and everything else, including Diazepam was stopped, stone dead. He was then crawling up the wall with electric shock pains in the head, so he was given Olanzapine. On top of this, also, 200 mg of Sertraline. His pain by then was unbearable, he had voids in his thinking, no one believed him, he was harangued for ‘attention-seeking behaviour’ by this same psychiatrist. Death had seemed the only way out. No hell could be worse than this.
The GMC asked our Lead Home Treatment psychiatrist to comment. For some months, he indicated that he might consider so doing. (He had disappeared for many months, on what we assumed to be ‘gardening leave’, after Olly’s suicide). The impression many of us had, was that he was playing games, pretending he would attend a GMC Hearing, but not really being serious about it. When at last the deadline for his submission came, he decided not to make one. None of the NHS witnesses to his brutality (social worker, doctor, student nurse) were called either. It was later admitted by the GMC in their report to us that his language had been somewhat out or order, but stopping the medications so suddenly, was not his problem. It was apparently Olly’s, for making the choice to follow his instructions! Here we go again with the word ‘choice’ which can be manipulated to remove all need for accountability.
So no, we don’t feel that the GMC care at all for ‘protecting patients from risk of harm posed by colleagues prescribing, administration or other errors.’ We think they are there to whitewash complaints away, and blame the patient at all times, leading us to feel that today doctors are ‘unaccountable god-like beings’ more fitted to be running a Police State, than to be interested in honesty when valid complaints are tentatively made by damaged patients, or parents of dead ones.
We shall continue to wave the AKATHISIA banner under noses everywhere. ‘We shall go down with the ship, there will be no white flag above our door’, in the words of one of Olly’s favourite songs by Dido. Except that unlike his, our ship is not going down any time soon, indeed, it’s taking on more passengers and proficient crew with every day that passes.
The GMC states: –
“Take responsibility for patient safety and quality of care”.
“You MUST take prompt action if you think that a patient’s safety, dignity or comfort is being seriously compromised”.
* If a patient is not receiving basic care to meet their needs, you MUST immediately tell someone who is in a position to act straight away.
*If patients are at risk because of inadequate premises, equipment or resources, policies or systems, you should put the matter right if that is possible.
You MUST raise your concerns in line with our guidance and your work place policy.
You should also make a record of the steps you have taken.
(My emphasis – as in GMC-speak, MUST offers no other option).
“If you have reason to believe that patients are, or may be, at risk of death or serious harm for any reason, you should report your concern to the appropriate person or organisation.
“You MUST not delay doing so because you are not in a position to put the matter right yourself”.
Clearly, a patient who’s psychiatrist has failed to diagnose AKATHISIA induced by their own or others prescriptions of SSRIs and other psychotropic drugs is by definition
“AT RISK OF DEATH” and has already suffered “SERIOUS HARM”.
“SAFETY DIGNITY AND COMFORT” have been destroyed, not only “COMPROMISED”.
The delivery of “care” by the kind of psychiatrist who creates terror, intimidation, command and control with vicious temper; combined with threats of detention and enforced treatment in patients and relatives, or career destruction in their staff, is the experience and cause of immense suffering to those who write on this site.
We have all seen, and been forced to endure this modus operandi, which is unlikely to be tolerated for long in any other field of medicine.
We know that the above, pious written words, are meaningless to such self-serving tyrants who “should never have been give a white coat”.
If the GMC wished to effectively make policy change that could rapidly and greatly improve patient safety, it MUST address the malignancy that is destroying medicine’s honour, integrity, and the trust of patients: that is: – Pharmaceutical conflicts of financial interest.
No doctor can prioritise safe prescribing and objectivity when receiving payment to promote pharmaceutical marketing policy, targets and objectives.
This is inarguably unethical, it must be addressed.
Tim.
It’s important to report the good as well as the bad. In my crusade to shout AKATHISIA from the rooftops, I visited my own GP today. I explained that we had been researching the reasons for our son’s death 4 years ago, (which he said he felt was totally sensible of us) and that we’d recently learnt about the enzyme CYP450 and that it now made sense to me why I had always had allergy type reactions to medications, anaphylactic shock to some, and akathisia from steroids in particular. He is a most approachable and intelligent man. He admitted that the word Akathisia was unknown to him, so I printed it on the list of medications I wanted him to add in the ‘warning pop up box’ on my Notes on his computer, which he unhesitatingly agreed to do.
We also discussed the doctor/patient relationship and balance of power – the nice cat sitting opposite the tremulous mouse, watching the swishing of the cat’s tail. I cited the example of my husband having been prescribed Cipro, our research and reluctance to take it, our dilemma over a weekend – ‘do we ask for something less strong as an antibiotic and risk enfuriating the prescriber, or does he take it and risk the awful limiting side effects, bearing in mind he is 77 and it’s contra-indicated for the over 60’s?’ In the end, we had asked for something else, actually over the phone from this very thoughtful GP (not the partner who had issued the prescription) and he advised waiting a while, which we did, and the infection cleared up itself.
So, I explained the fear of the patient, not wanting to alienate the GP but being wary of the side effects of medications in general. He said we would never upset him (except if we shouted at him – he said with a grin). His words were ‘it’s your body, when all is said and done, and it’s for you to decide what best to do for it, and I would always respect that. I might not share your views, but that is nothing to do with it.’
I also explained the akathisia our son had suffered, ever since the RoAccutane and Seroxat back in 2002/3, and told him in a nutshell what had happened in between. I explained the hell of anti-depressant and anti-psychotic induced akathisia, it’s not being recognised, and the inevitable endless circle of misjudged so-called ‘mental illness’. I stressed this was not about blame, it was about making sure others did not die after suffering the hellish existence that for 11 years, Olly had done. (In 2002/3 he was still their patient).
I felt that this GP really listened, cared, and did not dismiss anything I said. I managed to explain it all in 10 minutes flat, having rehearsed it in my mind all day. 🙂 So, one more influential human being now knows about AKATHISIA!
Wonderful to read Heather. Real consultation still exists.
An example to us all from sides of this doctor-patient interaction.
The process itself sounds to have been a therapeutic experience.
I do hope this doctor is teaching future GPs.
Tim.
An example to us all from both sides of this doctor-patient interaction.
I had to wait almost a month to get an appointment with this doctor. He is in his forties, I’d guess, in our large rural practice. The patients know who listens, and who is effective, so when they can, they wait for the best, tried and tested. Hence the long waiting list to see him! I don’t know whether doctors are aware how much patients exchange views in their communities about who is approachable and aids recovery, and who is best avoided. There are still one or two doctors in that Practice who were most unhelpful and made life very difficult for us all when our son was still their patient, living with us, when he first became ill on RoAccutane and Seroxat. We make sure we keep out of their way. One did apologise after his death, saying ‘we doctors do make mistakes sometimes….’
The interesting sequel to my good experience on Tuesday, will be when my husband sees another doctor in the Practice, (for whom there was not such a long wait) and asks her the same question, ‘does she know about AKATHISIA, and also the CYP450 enzyme’. It will be amazing if word has spread through the surgery yet. We will take with us some printed information, just in case. Totally agree Tim, I really hope that very professional man is doing some teaching of new GPs. His attitude is optimistic, smiling, welcoming, and yet he obviously listens carefully, and is never patronising. It was indeed therapeutic for me, and makes me feel very safe, to know he is there.
Perhaps your highly regarded G.P. could teach trainee psychiatrists?
a) How to achieve and maintain a therapeutic consultation.
b) That a therapeutic consultation would frequently be of far greater clinical value and recovery benefit than their ferrous wheel of increasingly toxic, psychotropic drugs. It is not a cause of life-threatening and life-taking ADRs.
c) That humility increases the patients trust and confidence in their doctor, enabling future therapeutic consultations to be readily achievable.
d) That this consultation process, between equals of different experience, is an infinitely more rewarding way to practice medicine and is also a defence against burn-out.
e) How to recognise AKATHISIA and thus avoid contributing to the tragic epidemic of iatrogenic, psychotropic induced, misdiagnosed “Serious Mental Illness”.
f) How to “actively listen” to patients, their families and loved ones.
g) That listening to patients is not only the foundation of safe and effective medical practice, it is also the best textbook of medicine.
h) That although empathy cannot be taught, it is possible to demonstrate to the trainee, that a vital and powerful therapeutic tool is available to the naturally empathetic doctor.
i) That saying sorry, when appropriate, enhances, rather than damages the doctor-patient relationship.
Sequel to attempts to raise AKATHISIA awareness in our local GP Practice: husband went to see new lady GP (as could not manage to wait a month for our usual one). This turned out to be a piece of good fortune. A very sensible listening and likeable person, who dealt with his health problem, and then, in the last minute or two, we told her about the death of our son. We asked her if she’d ever heard of AKATHISIA…..no, she hadn’t. We explained. She listened carefully. We offered our typed information – it was our updated Candle Vigil sheet, as used at the first WellBeing Hub meeting of NHS Providers. She accepted it eagerly and we feel sure she will read and absorb it; she said she is always terribly carefully about recommending the acne drug RoAccutane/isotretinoin to young patients, explaining the risks, and she feels the local hospital Dermatologist is careful too. (We’ve raised it with her a few months back and got a cool reception, have to say). We pointed out that the risk of possibly permanent sexual dysfunction is not listed on the PIL even though we admit, as she said, it does work to reduce the acne in most cases. It didn’t really work well for Olly’s acne and he had, over time, several courses and the acne always returned. We explained about his reactions to Seroxat. She listened.
So, on we go, another GP knows. It would have been amazing if word had already spread in that group Practice but coincidentally we passed our (star!) GP in the corridor on the way to see the new one, he said ‘hello?’ surprised to see husband on way to see someone other than he, so hopefully he will ask her later what was up. That may reinforce our point.
We have new targets next week, in a different field of care. Will report back with results.
At seminar for County health volunteers yesterday, further opportunity to explain AKATHISIA to all present, printed updated Candle Vigil sheet handed out by us None had, of course, heard of The Big A. One was an exGP (married to a practicing GP). Interestingly, she had stopped being a GP and was now energetically exploring arts courses and creativity in volunteering. Another lady had a background in pharmacy. Others were counsellers. All received information with interest. Discussion about SSRIs and anti-psychotics and CYP450. We described Dr Healy’s crusade and directed them to look at RxISK.org. All very positive.
On to the next…..
Excellent Heather, keep up the (very) good work and continue to keep us informed ……
I am thinking now of little acorns (plenty in my garden this autumn) and of the very tall, broad oak tree that stands there (the leaves have only just turned golden and begun to fall)
Knowledge of AKATHISIA is, I would suggest, not even an acorn yet, just one of the tiny blossom flowers* but it will be, and then, with determination, perseverance and patience will eventually become that oak tree known to all (at least all in the medical and caring professions and hopefully widespread amongst the general public)
No BigPharma ‘pesticide’ will dampen its growth!
* “on a flowering oak twig you have to look close to see the female flowers — the future acorns”
Thanks Jane, great idea, that ‘s what we need the acorns growing into trees, but we need fast growing ones because lives are being lost or ruined every minute of each day.
What about AKATHISIA banners, like our RoAccutane/isotretinoin banners, which we could unfurl in shopping centres and ask people if they knew what the word means? Maybe film the interviews. Give a small prize for anyone who can describe akathisia, what causes it, and what to do at once when it happens. A sort of First Aid exercise. We need to target people like St John’s Ambulance, and definitely the next on my list, The Samaritans. Then, MIND, Young Minds, A Place2Be, Rethink, we need a list. Any ideas anyone?
Our local NHS Trust has asked for volunteers to be….wait for it….
‘Quality Improvement Champions —-
Role description: this is a new and ground breaking initiative which aims to promote and embed the organisation’s quality aims and values’
There is a lot more health speak stuff, but at the bottom, a picture of a lion with the words
‘Take pride, lead others’, and ‘Become a Quality Improvement Champion, let’s hear your voice, let’s hear your ROAR’. Do we think they mean it?
Further thought, small prize can be small toy squirrel, clutching acorn. I can supply these. Message – ‘bounce the word around about AKATHISIA – save lives, from small acorns enormous things will grow.’
Squirrel will have ‘signs of akathisia’ and other useful RxISK info on small card, tucked up inside his tum, as he’ll be a little finger puppet.
Today’s challenge was excellent NHS physiotherapist, and she did know the word AKATHISIA thought it meant ‘withdrawal’, so I added the rest. She is a really enlightened physio, and I feel sure she’ll spread the word.